You might also like
- Anja Ainamo 1992 in His 18 Year Follow Up Study AfterDocument215 pagesAnja Ainamo 1992 in His 18 Year Follow Up Study AfterSuperna TiwariNo ratings yet
- 6 Surgical Periodontal TherapyDocument38 pages6 Surgical Periodontal TherapyPriya SargunanNo ratings yet
- FrenectomyDocument22 pagesFrenectomyPallav Ganatra100% (3)
- Horizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualFrom EverandHorizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualRating: 4.5 out of 5 stars4.5/5 (2)
- Contemporary Periodontal Surgery: An Illustrated Guide to the Art behind the ScienceFrom EverandContemporary Periodontal Surgery: An Illustrated Guide to the Art behind the ScienceNo ratings yet
- Periodontal Surgery Objectives and TechniquesDocument67 pagesPeriodontal Surgery Objectives and TechniquesShabeer Ali Abdul SalamNo ratings yet
- General Principles of Periodontal SurgeryDocument20 pagesGeneral Principles of Periodontal SurgerysevattapillaiNo ratings yet
- Ceramic Laminate Veneers: Clinical Procedures With A Multidisciplinary ApproachDocument23 pagesCeramic Laminate Veneers: Clinical Procedures With A Multidisciplinary ApproachBenjiNo ratings yet
- Simplified Papilla Preservation TechniqueDocument29 pagesSimplified Papilla Preservation TechniqueWendy JengNo ratings yet
- LECTURE ExodontiaDocument113 pagesLECTURE ExodontiaNuzhat Noor Ayesha89% (9)
- Periodontal Flap Surgery 2Document45 pagesPeriodontal Flap Surgery 2Emine Alaaddinoglu100% (2)
- Basic Surgical Techniques For Endosseous Implant PlacementDocument101 pagesBasic Surgical Techniques For Endosseous Implant PlacementAnshuman Dwivedi100% (2)
- RecessionsDocument68 pagesRecessionsmaryamNo ratings yet
- Indication To The Type of RestorationDocument61 pagesIndication To The Type of RestorationDr.O.R.GANESAMURTHINo ratings yet
- Immediate Implant Placement PDFDocument11 pagesImmediate Implant Placement PDFFerdinan PasaribuNo ratings yet
- Supportive Periodontal TreatmentDocument29 pagesSupportive Periodontal TreatmentAtul Koundel100% (2)
- GINGIVECTOMYDocument6 pagesGINGIVECTOMYFerdinan Pasaribu100% (1)
- Soft Tissue Recession Around ImplantsDocument8 pagesSoft Tissue Recession Around Implantsalexdental100% (1)
- Dental Bleaching Techniques for Lightening Tooth ColorDocument8 pagesDental Bleaching Techniques for Lightening Tooth ColorRiyan Adiputra Lukardi100% (1)
- Ebooks 10 Tips ImplantologyDocument16 pagesEbooks 10 Tips ImplantologylupusebastianNo ratings yet
- (IJPRD) GLUCKMAN 2017 - Partial Extraction Therapies Part 2 PDFDocument11 pages(IJPRD) GLUCKMAN 2017 - Partial Extraction Therapies Part 2 PDFFelipeGuzanskyMilaneziNo ratings yet
- Clinical Photography Part - 2 PDFDocument3 pagesClinical Photography Part - 2 PDFsonal agarwalNo ratings yet
- Periodontal FlapsDocument65 pagesPeriodontal FlapsSaleh AlsadiNo ratings yet
- Bringing Back Quality Smiles With Dental ImplantsDocument145 pagesBringing Back Quality Smiles With Dental ImplantsAmar Bimavarapu100% (2)
- Amalgam RestorationsDocument36 pagesAmalgam Restorationsdrshivanim100% (1)
- VeneersDocument50 pagesVeneersDr FarhatNo ratings yet
- Critical Soft-Tissue Dimensions With Dental Implantsand Treatment Concepts PDFDocument13 pagesCritical Soft-Tissue Dimensions With Dental Implantsand Treatment Concepts PDFgirl33No ratings yet
- Classification of Dental CariesDocument79 pagesClassification of Dental Cariesmarukala100% (1)
- Naturally Aesthetic Restorations and Minimally Invasive DentistryDocument12 pagesNaturally Aesthetic Restorations and Minimally Invasive Dentistrynataly2yoNo ratings yet
- Prosthetic Aspects of Dental Implants - IIDocument73 pagesProsthetic Aspects of Dental Implants - IIKomal TalrejaNo ratings yet
- Esthetics in Dental ImplantsDocument87 pagesEsthetics in Dental ImplantsRavi Uttara100% (3)
- Socket PreservationDocument8 pagesSocket PreservationManu Gupta0% (1)
- (RestoDent) Components of Cavity PrepDocument47 pages(RestoDent) Components of Cavity PrepZara Sebastianne GarciaNo ratings yet
- Perio Restorative Inter Relationship II PerioDocument48 pagesPerio Restorative Inter Relationship II PerioFourthMolar.com100% (2)
- Aesthetic and Cosmetic Dentistry Made Easy, 1ed (2008) PDFDocument103 pagesAesthetic and Cosmetic Dentistry Made Easy, 1ed (2008) PDFDaniel RapcauNo ratings yet
- EW Step by Step Veneer enDocument5 pagesEW Step by Step Veneer enVipul SrivastavaNo ratings yet
- Periodontal disease and systemic healthDocument145 pagesPeriodontal disease and systemic healthAkash Yss Boddeda50% (2)
- Ridge AugmentationDocument109 pagesRidge AugmentationSingh Jyoti100% (3)
- Anita Kapri: Keyword: Smile Makeover, Digital Smile Design, EstheticsDocument8 pagesAnita Kapri: Keyword: Smile Makeover, Digital Smile Design, Estheticsalaesa2007No ratings yet
- Basic Surgical Principle in ImplantologyDocument19 pagesBasic Surgical Principle in ImplantologyMaryam ZanjirNo ratings yet
- Digital Dental Photography HandoutDocument41 pagesDigital Dental Photography HandoutMarius Oprișor100% (2)
- Principles of Designing Mucoperiosteal FlapsDocument70 pagesPrinciples of Designing Mucoperiosteal FlapsStephen KinyanjuiNo ratings yet
- Prostho IV - Slide 3 - Impression - Making - For - Complete - DenturesDocument82 pagesProstho IV - Slide 3 - Impression - Making - For - Complete - Denturesبراءة أحمد السلامات100% (1)
- Gingivectomy and Gingivoplasty: DisadvantagesDocument7 pagesGingivectomy and Gingivoplasty: Disadvantageskarolys1994100% (1)
- Minor Oral Surgical Principles (NXPowerLite) / Orthodontic Courses by Indian Dental AcademyDocument42 pagesMinor Oral Surgical Principles (NXPowerLite) / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Suturing Techniques in Periodontal Plastic SurgeryDocument9 pagesSuturing Techniques in Periodontal Plastic SurgeryNishtha Kumar100% (1)
- JC Laminates VeneersDocument47 pagesJC Laminates Veneersvarsha palledNo ratings yet
- Over Dentures Jan 2012Document40 pagesOver Dentures Jan 2012Mohsin HabibNo ratings yet
- Iti Implant Course 2018 PDFDocument5 pagesIti Implant Course 2018 PDFShyam K MaharjanNo ratings yet
- Root Coverage Procedures SantDocument22 pagesRoot Coverage Procedures SantPrasun Sit SharmaNo ratings yet
- Basic Dental Implant SurgeryDocument33 pagesBasic Dental Implant Surgerymuhammad100% (1)
- Innovations in EndodonticsDocument14 pagesInnovations in EndodonticsLeHoaiNo ratings yet
- Anterior Implant EstheticsDocument9 pagesAnterior Implant EstheticsRatih Cynthia100% (1)
- Periodontal Flap Surgery Techniques and ConsiderationsDocument38 pagesPeriodontal Flap Surgery Techniques and ConsiderationsChauhan Naresh100% (1)
- Working Length DeterminationDocument97 pagesWorking Length Determinationrolly_jatinNo ratings yet
- Occlusal Adjustment Technique Made Simple: Masticatory System and Occlusion As It Relates to Function and How Occlusal Adjustment Can Help Treat Primary and Secondary Occlusal TraumaFrom EverandOcclusal Adjustment Technique Made Simple: Masticatory System and Occlusion As It Relates to Function and How Occlusal Adjustment Can Help Treat Primary and Secondary Occlusal TraumaNo ratings yet
- Avoiding and Treating Dental Complications: Best Practices in DentistryFrom EverandAvoiding and Treating Dental Complications: Best Practices in DentistryDeborah A. TermeieNo ratings yet
- MRNA Vaccines, A New Era-Cytiva-2022Document29 pagesMRNA Vaccines, A New Era-Cytiva-2022Arturo Manzo-FontesNo ratings yet
- Rak Bishop BasimaDocument5 pagesRak Bishop BasimafrossNo ratings yet
- GQGH PresentationDocument26 pagesGQGH Presentationapi-559575515No ratings yet
- Interpretive Summary: Mean Cell Volume (MCV)Document2 pagesInterpretive Summary: Mean Cell Volume (MCV)Wael SafwatNo ratings yet
- Safety Data Sheet for perma Multipurpose grease SF01Document7 pagesSafety Data Sheet for perma Multipurpose grease SF01Singgih KurniawanNo ratings yet
- FlowerhornDocument10 pagesFlowerhornPaul Michael P. GarciaNo ratings yet
- 17425247.20113. Oral Formulation StrategiesDocument18 pages17425247.20113. Oral Formulation StrategiesPaqui Miranda GualdaNo ratings yet
- Housing Inequality Causes and SolutionsDocument5 pagesHousing Inequality Causes and SolutionsFredrickNo ratings yet
- Philosophy Essay on Beauty StandardsDocument8 pagesPhilosophy Essay on Beauty StandardsMafe DeoroNo ratings yet
- Types of Appraisals and ReviewsDocument22 pagesTypes of Appraisals and ReviewsJon ColenNo ratings yet
- Phytochemical Screening and in Vitro Antibacterial Activities of The Ethanol Extract of Vernonia Amygdalina Bitter Leaf On Staphylococcus AureusDocument6 pagesPhytochemical Screening and in Vitro Antibacterial Activities of The Ethanol Extract of Vernonia Amygdalina Bitter Leaf On Staphylococcus AureusEditor IJTSRDNo ratings yet
- Huntington's DiseaseDocument17 pagesHuntington's DiseaseJia HuiNo ratings yet
- Persona The Personalized Knee Surgical TechniqueDocument76 pagesPersona The Personalized Knee Surgical TechniqueBIG JasonNo ratings yet
- New GHPL Claim Form PDFDocument3 pagesNew GHPL Claim Form PDFp_srib4uNo ratings yet
- ESIC DespenseriesDocument6 pagesESIC DespenseriesAbcxyz XyzabcNo ratings yet
- Impact of Covid 19 Mental Health SynopsisDocument7 pagesImpact of Covid 19 Mental Health SynopsisNikita ChaubeNo ratings yet
- Autism and Schizophrenia Intestinal Disorders Cade2000Document17 pagesAutism and Schizophrenia Intestinal Disorders Cade2000Armando CottimNo ratings yet
- Doctors Note For Absence Return To WorkDocument2 pagesDoctors Note For Absence Return To WorkMolly ClarkNo ratings yet
- DLL Ls2 Reproductive SystemDocument4 pagesDLL Ls2 Reproductive SystemAurora Corea AbanNo ratings yet
- 6allergic Reactions To CosmeticsDocument2 pages6allergic Reactions To Cosmeticsnendra19No ratings yet
- MGMT 6250 D01 SyllabusDocument5 pagesMGMT 6250 D01 SyllabusSamantha RomanowskiNo ratings yet
- Mcintyre, John 04/13/1990 Patient ReportDocument7 pagesMcintyre, John 04/13/1990 Patient ReportJohn McIntyreNo ratings yet
- Learning Continuity Plan for Education in the Time of COVID-19Document65 pagesLearning Continuity Plan for Education in the Time of COVID-19Earls jr Computer100% (1)
- Highway ImportantDocument1 pageHighway ImportantArun Sethi100% (1)
- MNG Charel 2Document97 pagesMNG Charel 2Kyrel Ann B. MadriagaNo ratings yet
- Bernardino Ramazzini's Early Observations of The Link Between Musculoskeletal Disorders and Ergonomic FactorsDocument4 pagesBernardino Ramazzini's Early Observations of The Link Between Musculoskeletal Disorders and Ergonomic FactorsJOSE JAVIER BARZALLO GALVEZNo ratings yet
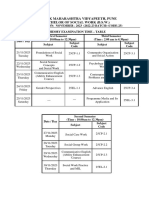
- BSW and MSW Exam Time Table For External and Regular November-2023 ExamDocument9 pagesBSW and MSW Exam Time Table For External and Regular November-2023 ExamashwinishyamthakarNo ratings yet
- RPMS Implementation in DepEd Aklan SchoolsDocument7 pagesRPMS Implementation in DepEd Aklan SchoolsRenwen LataNo ratings yet
- MC 3 Lab - KerolDocument43 pagesMC 3 Lab - KerolMa Carolin De LeonNo ratings yet
- Newfoundland Labrador Skin and Wound Care ManualDocument135 pagesNewfoundland Labrador Skin and Wound Care ManualBrian HarrisNo ratings yet