You might also like
- Adult onset Rasmussen's syndrome presenting with psychosisDocument7 pagesAdult onset Rasmussen's syndrome presenting with psychosisBalasubrahmanya K. R.No ratings yet
- The Personal Disturbance Scale (Dssi/Sad) : Development, Use and StructureDocument18 pagesThe Personal Disturbance Scale (Dssi/Sad) : Development, Use and StructureBalasubrahmanya K. R.100% (1)
- Temperament PDFDocument4 pagesTemperament PDFBalasubrahmanya K. R.No ratings yet
- 5 Steps To Make Retirement Years Happier For Your ParentsDocument6 pages5 Steps To Make Retirement Years Happier For Your ParentsBalasubrahmanya K. R.No ratings yet
- Functional Nausea and VomitingDocument4 pagesFunctional Nausea and VomitingBalasubrahmanya K. R.No ratings yet
- Indian Bank ChallanDocument1 pageIndian Bank ChallanBalasubrahmanya K. R.No ratings yet
- 1400 Calories Indian Diet Plan For Weight LossDocument11 pages1400 Calories Indian Diet Plan For Weight LossBalasubrahmanya K. R.0% (1)
- Dynamic Psychoth For Personality DisordDocument285 pagesDynamic Psychoth For Personality DisordPetzyMarian100% (1)
- Paternal Postnatal Psychiatric - IllnessesDocument202 pagesPaternal Postnatal Psychiatric - IllnessesBalasubrahmanya K. R.No ratings yet
- How To Open National Pension Scheme (ENPS) Online and OfflineDocument7 pagesHow To Open National Pension Scheme (ENPS) Online and OfflineBalasubrahmanya K. R.No ratings yet
- 1400 Calories Indian Diet Plan For Weight LossDocument11 pages1400 Calories Indian Diet Plan For Weight LossBalasubrahmanya K. R.0% (1)
- Q PlastyDocument4 pagesQ PlastyBalasubrahmanya K. R.No ratings yet
- How To Open National Pension Scheme (ENPS) Online and OfflineDocument7 pagesHow To Open National Pension Scheme (ENPS) Online and OfflineBalasubrahmanya K. R.No ratings yet
- MRCpsych 2016 CalendarDocument2 pagesMRCpsych 2016 CalendarBalasubrahmanya K. R.No ratings yet
- Statistics NotesDocument15 pagesStatistics NotesBalasubrahmanya K. R.No ratings yet
- A Proposed Diagnostic Scheme For People With Epileptic SeizuresDocument9 pagesA Proposed Diagnostic Scheme For People With Epileptic SeizuresBalasubrahmanya K. R.No ratings yet
- International Study of The Relation Between Somatic Symptoms and DepressionDocument7 pagesInternational Study of The Relation Between Somatic Symptoms and DepressionBalasubrahmanya K. R.No ratings yet
- DementiaDocument15 pagesDementiaBalasubrahmanya K. R.No ratings yet
- Suicide PreventionDocument2 pagesSuicide PreventionBalasubrahmanya K. R.No ratings yet
- cds2 2012 EngDocument9 pagescds2 2012 Engsur22961No ratings yet
- P 007 OlanzapineDocument11 pagesP 007 OlanzapineBalasubrahmanya K. R.No ratings yet
- Neet StuffDocument26 pagesNeet StuffBalasubrahmanya K. R.No ratings yet
- Factors Contributing To The Stigma of EpilepsyDocument7 pagesFactors Contributing To The Stigma of EpilepsyAbhishek SāmalNo ratings yet
- Harvard Reference GuideDocument16 pagesHarvard Reference GuideBalasubrahmanya K. R.No ratings yet
- Prevalence of Met Synd in Mood Disorder and Psychosis in Pts.Document7 pagesPrevalence of Met Synd in Mood Disorder and Psychosis in Pts.Balasubrahmanya K. R.No ratings yet
- Psychopathology Consensus StatementDocument8 pagesPsychopathology Consensus Statementscabrera_scribdNo ratings yet
- Interventions in EM StudyDocument12 pagesInterventions in EM StudyBalasubrahmanya K. R.No ratings yet
- Cross-Cultural Differences in IQ Test Performance: Extension of An Existing Normative Database On WAIS-III Test PerformanceDocument79 pagesCross-Cultural Differences in IQ Test Performance: Extension of An Existing Normative Database On WAIS-III Test PerformanceBalasubrahmanya K. R.No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chapter 2 EnglishDocument9 pagesChapter 2 Englishdgdhdh_66No ratings yet
- (Macmillan Studies in Marketing Management) Frank Jefkins BSC (Econ), BA (Hons), MCAM, FIPR, MInstM, MAIE, ABC (Auth.) - Public Relations For Marketing Management-Palgrave Macmillan UK (1983)Document193 pages(Macmillan Studies in Marketing Management) Frank Jefkins BSC (Econ), BA (Hons), MCAM, FIPR, MInstM, MAIE, ABC (Auth.) - Public Relations For Marketing Management-Palgrave Macmillan UK (1983)Subhasis DasNo ratings yet
- Vandergrift - Listening, Modern Theory & PracticeDocument6 pagesVandergrift - Listening, Modern Theory & PracticeKarolina CiNo ratings yet
- I-Plan Marketing List On Installments 11-Aug-23Document10 pagesI-Plan Marketing List On Installments 11-Aug-23HuxaifaNo ratings yet
- Daraz PKDocument4 pagesDaraz PKshavais100% (1)
- Effective Postoperative Pain Management StrategiesDocument10 pagesEffective Postoperative Pain Management StrategiesvenkayammaNo ratings yet
- 28/08/2016 1 Advanced Research Methodology... RU, Bangalore-64Document38 pages28/08/2016 1 Advanced Research Methodology... RU, Bangalore-64Ananthesh RaoNo ratings yet
- Action and Budget Plan For The Boys Scouts of The PhilippinesDocument2 pagesAction and Budget Plan For The Boys Scouts of The PhilippinesJohn Paul ViñasNo ratings yet
- R-101 and D-101 energy balancesDocument4 pagesR-101 and D-101 energy balancesPuteri MimieNo ratings yet
- Revised Pharmacophore Model For 5 HT2A Receptor Antagonists Derived From The Atypical Antipsychotic Agent RisperidoneDocument14 pagesRevised Pharmacophore Model For 5 HT2A Receptor Antagonists Derived From The Atypical Antipsychotic Agent RisperidoneLUCAS OYANEDERNo ratings yet
- Populist Movement (Anant)Document7 pagesPopulist Movement (Anant)Siddhi JoshiNo ratings yet
- The 4Ms of Operations: Prepared By: Karla Jane F. BangaysisoDocument18 pagesThe 4Ms of Operations: Prepared By: Karla Jane F. BangaysisoKarla BangFerNo ratings yet
- Semi Detailed Lesson Format BEEd 1Document2 pagesSemi Detailed Lesson Format BEEd 1Kristine BuenaventuraNo ratings yet
- Haley Sue Exsted FacebookDocument58 pagesHaley Sue Exsted Facebookapi-323808402No ratings yet
- Responsibility Matrix D&B Rev 3 22 - Sep - 2014Document10 pagesResponsibility Matrix D&B Rev 3 22 - Sep - 2014hatemsharkNo ratings yet
- Product Placement in Movies- Impact on SalesDocument3 pagesProduct Placement in Movies- Impact on SalesBhavya DiddeeNo ratings yet
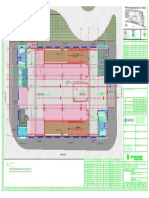
- Key plan and area statement comparison for multi-level car park (MLCPDocument1 pageKey plan and area statement comparison for multi-level car park (MLCP121715502003 BOLLEMPALLI BINDU SREE SATYANo ratings yet
- Nothophytophthora Gen. Nov., A New Sister Genus of Phytophthora From Natural and Semi-Natural Ecosystems in Europe, Chile and VietnamDocument32 pagesNothophytophthora Gen. Nov., A New Sister Genus of Phytophthora From Natural and Semi-Natural Ecosystems in Europe, Chile and VietnamChi Nguyen MinhNo ratings yet
- Engineering Standard for Rolling Stock Minimum In-Service ConditionsDocument19 pagesEngineering Standard for Rolling Stock Minimum In-Service Conditions4493464No ratings yet
- Assessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale EvaluationDocument9 pagesAssessment Nursing Diagnosis Scientific Rationale Planning Intervention Rationale Evaluationclydell joyce masiarNo ratings yet
- Ammonium Nitrophosphate Production ProcessDocument133 pagesAmmonium Nitrophosphate Production ProcessHit Busa100% (1)
- Ball Bearings 1Document17 pagesBall Bearings 1ManicharanNo ratings yet
- Porter 5 ForcesDocument44 pagesPorter 5 ForcesSwapnil ChonkarNo ratings yet
- Rate of Change: Example 1 Determine All The Points Where The Following Function Is Not ChangingDocument5 pagesRate of Change: Example 1 Determine All The Points Where The Following Function Is Not ChangingKishamarie C. TabadaNo ratings yet
- VPN Risk Report Cybersecurity InsidersDocument20 pagesVPN Risk Report Cybersecurity InsidersMaria PerezNo ratings yet
- Build A Tunnel: What You NeedDocument2 pagesBuild A Tunnel: What You NeedManila Business ShopsNo ratings yet
- Grade 5 PPT English Q4 W3 Day 2Document17 pagesGrade 5 PPT English Q4 W3 Day 2Rommel MarianoNo ratings yet
- Eslit-Vinea-LA 03 Task #1-4Document11 pagesEslit-Vinea-LA 03 Task #1-4darkNo ratings yet
- B. Com II Year Economics Previous Year QuestionsDocument11 pagesB. Com II Year Economics Previous Year QuestionsShashiMohanKotnalaNo ratings yet
- Cost Accounting DQ - Midterms - AnswersDocument10 pagesCost Accounting DQ - Midterms - AnswersKurt dela TorreNo ratings yet