You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Comparison of Fine Needle Aspiration Cytology (FNAC) and Histopathology in The Diagnosis of Neck MassesDocument4 pagesComparison of Fine Needle Aspiration Cytology (FNAC) and Histopathology in The Diagnosis of Neck MassesSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- A Crossectional Study of Glycosylated Haemoglobin (HbA1c) Values in Type II Diabetes Mellitus & Its Relationship With Lipid Profile and Diabetes ComplicationsDocument3 pagesA Crossectional Study of Glycosylated Haemoglobin (HbA1c) Values in Type II Diabetes Mellitus & Its Relationship With Lipid Profile and Diabetes ComplicationsSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Study of Pneumoconiosis in Thermal Power Station WorkersDocument4 pagesStudy of Pneumoconiosis in Thermal Power Station WorkersSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Why and How Aerobic Mesophilic Composting Is Effective A Comprehensive Study On Aerobic and Anaerobic Composting of Green Waste Under Mesophilic and Thermophilic ConditionDocument7 pagesWhy and How Aerobic Mesophilic Composting Is Effective A Comprehensive Study On Aerobic and Anaerobic Composting of Green Waste Under Mesophilic and Thermophilic ConditionSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Maternal Risk Factors Determining Birth Weight of Newborns A Tertiary Care Hospital Based StudyDocument6 pagesMaternal Risk Factors Determining Birth Weight of Newborns A Tertiary Care Hospital Based StudySTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Efficiency of Neighbour Balanced Block Designs For Correlated ObservationsDocument6 pagesEfficiency of Neighbour Balanced Block Designs For Correlated ObservationsSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Control of Chaos in Some Non Linear MapsDocument6 pagesControl of Chaos in Some Non Linear MapsSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Self-Health Care Practices Among Type 2 Diabetes Patients Attending Diabetes Clinic in India A Descriptive Cross-Sectional StudDocument4 pagesSelf-Health Care Practices Among Type 2 Diabetes Patients Attending Diabetes Clinic in India A Descriptive Cross-Sectional StudSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Correlation of Alpha-1 Antitrypsin and Smoking in Chronic Obstructive Lung DiseaseDocument4 pagesCorrelation of Alpha-1 Antitrypsin and Smoking in Chronic Obstructive Lung DiseaseSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Crossectional Study of VO2max and Plasma Lactate Values in Football PlayersDocument5 pagesA Crossectional Study of VO2max and Plasma Lactate Values in Football PlayersSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On πgβ-Closed sets in Topological SpacesDocument1 pageOn πgβ-Closed sets in Topological SpacesSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- An Integrative Approach Towards Conceptual Frameworks For Injury PreventionDocument4 pagesAn Integrative Approach Towards Conceptual Frameworks For Injury PreventionSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Assessment of Groundwater Quality and Its Suitability For Drinking Uses in Warora Tehsil, District Chandrapur, IndiaDocument5 pagesAssessment of Groundwater Quality and Its Suitability For Drinking Uses in Warora Tehsil, District Chandrapur, IndiaSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- An Integrative Approach Towards Conceptual Frameworks For Injury PreventionDocument4 pagesAn Integrative Approach Towards Conceptual Frameworks For Injury PreventionSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Statistical Study of Evaluation of The Relationship Between Students' Involvements in NSS Based On Extracurricular Activities and Their Achievement in Mathematical SciencesDocument6 pagesA Statistical Study of Evaluation of The Relationship Between Students' Involvements in NSS Based On Extracurricular Activities and Their Achievement in Mathematical SciencesSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Morphology, Occurrence, Natural Habitat, Structure and Texture of GeastrumDocument3 pagesMorphology, Occurrence, Natural Habitat, Structure and Texture of GeastrumSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Half-Cauchy Distribution and ProcessDocument5 pagesOn Half-Cauchy Distribution and ProcessSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Study of CNS Infections in HIV Positive PatientsDocument6 pagesStudy of CNS Infections in HIV Positive PatientsSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- A Statistical Study of Evaluation of The Relationship Between Students' Involvements in NSS Based On Extracurricular Activities and Their Achievement in Mathematical SciencesDocument6 pagesA Statistical Study of Evaluation of The Relationship Between Students' Involvements in NSS Based On Extracurricular Activities and Their Achievement in Mathematical SciencesSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Squeeze Film Lubrication Between Parallel Stepped Plates With Couplestress FluidsDocument5 pagesSqueeze Film Lubrication Between Parallel Stepped Plates With Couplestress FluidsSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Hydromagnetic Oscillatory Flow Through A Porous Channel in The Presence of Hall Current With Variable Suction and PermeabilityDocument7 pagesHydromagnetic Oscillatory Flow Through A Porous Channel in The Presence of Hall Current With Variable Suction and PermeabilitySTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Control of Rat Population Through Bhelwa Oil in Panch - Pargana Area of JharkhandDocument2 pagesControl of Rat Population Through Bhelwa Oil in Panch - Pargana Area of JharkhandSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Progesterone Hydrotherapy in Management of Small, Mid and Lower Ureteric CalculiDocument4 pagesProgesterone Hydrotherapy in Management of Small, Mid and Lower Ureteric CalculiSTATPERSON PUBLISHING CORPORATION100% (1)
- MV - Optimality of Nearest Neighbour Balanced Block Designs Using First Order and Second Order Correlated ModelsDocument4 pagesMV - Optimality of Nearest Neighbour Balanced Block Designs Using First Order and Second Order Correlated ModelsSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- On The Extension of Topological Local Groups With Local Cross SectionDocument6 pagesOn The Extension of Topological Local Groups With Local Cross SectionSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Food Selection Acceptance Activities For Promoting Pro-Vitamin A Foods Among Young Children in Urban SlumsDocument3 pagesFood Selection Acceptance Activities For Promoting Pro-Vitamin A Foods Among Young Children in Urban SlumsSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Determination of Expected Time To Seroconversion When The Antigenic Diversity Threshold Follows Order StatisticDocument5 pagesDetermination of Expected Time To Seroconversion When The Antigenic Diversity Threshold Follows Order StatisticSTATPERSON PUBLISHING CORPORATIONNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Growth and Development of Cleft Lip and Cleft Palate Children Before and After Reconstruction SurgeryDocument4 pagesGrowth and Development of Cleft Lip and Cleft Palate Children Before and After Reconstruction SurgerySTATPERSON PUBLISHING CORPORATIONNo ratings yet
- Improving Outcome in Tracheostomy Our StudyDocument7 pagesImproving Outcome in Tracheostomy Our StudySTATPERSON PUBLISHING CORPORATIONNo ratings yet
- List of Grocery Importers in Austria Europe PDF FreeDocument11 pagesList of Grocery Importers in Austria Europe PDF FreeEmpy SumardiNo ratings yet
- Ions & Ionic Bonds (Multiple Choice) QPDocument7 pagesIons & Ionic Bonds (Multiple Choice) QPBăng Băng LêNo ratings yet
- WaveLab - BUC Datasheet - Ku Band 80W 100WDocument4 pagesWaveLab - BUC Datasheet - Ku Band 80W 100WLeonNo ratings yet
- Mini Dental ImplantsDocument11 pagesMini Dental ImplantsDario PuljićNo ratings yet
- 3RD Summative Exam in Science 6Document6 pages3RD Summative Exam in Science 6Maricris Palermo SancioNo ratings yet
- Account Transfer Form: Fax Cover SheetDocument6 pagesAccount Transfer Form: Fax Cover SheetJitendra SharmaNo ratings yet
- Karen Horney's Theories of PersonalityDocument8 pagesKaren Horney's Theories of PersonalityGeorge BaywongNo ratings yet
- 150.66-RP4 YcalDocument92 pages150.66-RP4 YcalJosé RamosNo ratings yet
- Worksheet. 5. Sexual Reproduction in PlantDocument4 pagesWorksheet. 5. Sexual Reproduction in PlantLeonita SwandjajaNo ratings yet
- Effects of Career Plateau On Job Satisfaction and MotivationDocument105 pagesEffects of Career Plateau On Job Satisfaction and Motivationalanwil100% (1)
- Midterm Requirement-Green BuildingDocument7 pagesMidterm Requirement-Green BuildingJo-anne RiveraNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Service ProgramDocument47 pagesService ProgramHuseyn aliyevNo ratings yet
- Labour Market Regimes V4.0Document8 pagesLabour Market Regimes V4.0Gail WardNo ratings yet
- Dr. Ashraf Sayeed: Department of OphthalmologyDocument49 pagesDr. Ashraf Sayeed: Department of Ophthalmologysaiful haque100% (1)
- Technical Documentation IPM: Savina 300 Intensive Care VentilatorDocument166 pagesTechnical Documentation IPM: Savina 300 Intensive Care VentilatorhoudaNo ratings yet
- Physical, Biology and Chemical Environment: Its Effect On Ecology and Human HealthDocument24 pagesPhysical, Biology and Chemical Environment: Its Effect On Ecology and Human Health0395No ratings yet
- Lab 2 - Capacitive ReactanceDocument4 pagesLab 2 - Capacitive Reactanceali basitNo ratings yet
- Production & Downstream Processing of Baker's Best FriendDocument26 pagesProduction & Downstream Processing of Baker's Best FriendMelissaNo ratings yet
- Midterm and Final Exam TFNDocument6 pagesMidterm and Final Exam TFNalchriwNo ratings yet
- History of Some Special ExplosivesDocument24 pagesHistory of Some Special ExplosivesShazil KhanNo ratings yet
- New Fda Nutrition Label Guidelines For Food ManufacturersDocument17 pagesNew Fda Nutrition Label Guidelines For Food ManufacturersSurendra RamkissoonNo ratings yet
- ADPKDDocument75 pagesADPKDVenkataramanan KrishnamoorthyNo ratings yet
- Microcosmic Orbit Breath Awareness and Meditation Process: For Enhanced Reproductive Health, An Ancient Taoist MeditationDocument1 pageMicrocosmic Orbit Breath Awareness and Meditation Process: For Enhanced Reproductive Health, An Ancient Taoist MeditationSaimon S.M.No ratings yet
- Nath Bio-Genes at Inflection Point-2Document9 pagesNath Bio-Genes at Inflection Point-2vinodtiwari808754No ratings yet
- Korean Wellhead KWM-2014-Revision0Document20 pagesKorean Wellhead KWM-2014-Revision0DrakkarNo ratings yet
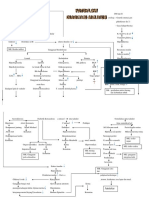
- Patoflow DMDocument2 pagesPatoflow DMAngel da CostaNo ratings yet
- Comparative Study of Different Varieties of Rice For Making Homemade Instant CoffeeDocument9 pagesComparative Study of Different Varieties of Rice For Making Homemade Instant CoffeeJhon Kyle RoblesNo ratings yet
- Reading Passage 1: IELTS Recent Actual Test With Answers Volume 1Document17 pagesReading Passage 1: IELTS Recent Actual Test With Answers Volume 1Amogha GadkarNo ratings yet
- Lactic AcidDocument6 pagesLactic AcidTaha AzNo ratings yet
- Labor To DigestDocument32 pagesLabor To Digestphoenix rogueNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- Breaking the Habit of Being YourselfFrom EverandBreaking the Habit of Being YourselfRating: 4.5 out of 5 stars4.5/5 (1457)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)