You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Correcting Forward HeadDocument64 pagesCorrecting Forward HeadPaul DoneyNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- History Cs Admitting Notes: + 10 "U" Oxytocin X 8 HDocument7 pagesHistory Cs Admitting Notes: + 10 "U" Oxytocin X 8 HKarl Martin PinedaNo ratings yet
- Patient Monitoring1370Document53 pagesPatient Monitoring1370Ridha Surya NugrahaNo ratings yet
- Non-Invasive, External Ultrasonic LipolysisDocument5 pagesNon-Invasive, External Ultrasonic LipolysisdoctorbanNo ratings yet
- NursingDocument136 pagesNursingMohammed Ahmed100% (1)
- Anaesthetic ServicesDocument169 pagesAnaesthetic ServicesMohammed AhmedNo ratings yet
- Adult Tachycardia Algorithm: (With Pulse)Document1 pageAdult Tachycardia Algorithm: (With Pulse)Mohammed AhmedNo ratings yet
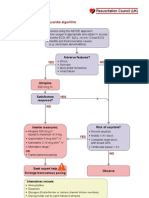
- Adult Bradycardia Algorithm: Adverse Features?Document1 pageAdult Bradycardia Algorithm: Adverse Features?Mohammed AhmedNo ratings yet
- Introduction To DentistryDocument13 pagesIntroduction To DentistryDr-Rmz RabadiNo ratings yet
- Technical Report 112Document47 pagesTechnical Report 112Julliane OrtizNo ratings yet
- ExEm Foam Kit New Folder HighResolution 20 Jan 2011Document2 pagesExEm Foam Kit New Folder HighResolution 20 Jan 2011Repede FlorentinaNo ratings yet
- 04 Endometrial PathologyDocument18 pages04 Endometrial Pathologylearta100% (1)
- Vodic Kroz Porodjaj 2Document33 pagesVodic Kroz Porodjaj 2NikolinaNo ratings yet
- MemoDocument18 pagesMemoAsad ZahidiNo ratings yet
- Quiz 1 AntepardumDocument2 pagesQuiz 1 Antepardumchase nicholsNo ratings yet
- Spacemed ArticleDocument4 pagesSpacemed ArticleBingDelaCruzNo ratings yet
- Butuan Doctors' College: O.R. Scrub Form MajorDocument4 pagesButuan Doctors' College: O.R. Scrub Form MajorNheljane DelacruzNo ratings yet
- Application For Medical X Ray FacilityDocument3 pagesApplication For Medical X Ray FacilitySALVADOR R. ENCINAS DISTRICT HOSPITALNo ratings yet
- Information Memorandum - 25 09 14 PDFDocument58 pagesInformation Memorandum - 25 09 14 PDFBogdan RosuNo ratings yet
- Ayushman Bharat:: Comprehensive Primary Health Care Through Health and Wellness CentersDocument96 pagesAyushman Bharat:: Comprehensive Primary Health Care Through Health and Wellness CentersSiva SaranNo ratings yet
- D1 - Theraputic Guidelines in Neonatal InfectionDocument15 pagesD1 - Theraputic Guidelines in Neonatal InfectiongaasheNo ratings yet
- Perioperative Nursing Care IssuesDocument7 pagesPerioperative Nursing Care IssuesAziil LiizaNo ratings yet
- Prenatal Care Routine Full Version 2Document98 pagesPrenatal Care Routine Full Version 2Devendra SonawaneNo ratings yet
- Unit 3 Hospital Staffs and Departments: Objectives: After The Lesson, Students Will Be Able ToDocument22 pagesUnit 3 Hospital Staffs and Departments: Objectives: After The Lesson, Students Will Be Able ToLinh TrầnNo ratings yet
- Daily Objectives: San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument2 pagesDaily Objectives: San Francisco St. Butuan City 8600, Region XIII Caraga, Philippinesako at ang exoNo ratings yet
- Voluson 730 Pro V BrochureDocument4 pagesVoluson 730 Pro V BrochureYolanda PeñaNo ratings yet
- Licensing Requirement For Acute-Chronic Psychiatric Facility - DOHDocument3 pagesLicensing Requirement For Acute-Chronic Psychiatric Facility - DOHAgnes Cheverloo CastilloNo ratings yet
- Self Applied Topical Fluorides ClassDocument23 pagesSelf Applied Topical Fluorides ClassultraswamyNo ratings yet
- Abnormal PueperiumDocument24 pagesAbnormal Pueperiumvvmounika reddy907No ratings yet
- Final Year QN Papers (1990-2017)Document37 pagesFinal Year QN Papers (1990-2017)vardhan hhh100% (4)
- Info DcsDocument9 pagesInfo DcsKhei Laqui SNNo ratings yet
- Kentucky Board of NursingDocument4 pagesKentucky Board of NursingZilbran BerontaxNo ratings yet
- Braxton Hicks or True Labor ContractionsDocument2 pagesBraxton Hicks or True Labor ContractionsJellyAnnGomezNo ratings yet