You might also like
- Medsolutions PharmacologyDocument123 pagesMedsolutions Pharmacologykamran_zarrarNo ratings yet
- Regional Anesthesia in TraumaDocument10 pagesRegional Anesthesia in TraumaClaudia Cruz AyalaNo ratings yet
- Nitrous Oxide and The Inhalation AnestheticsDocument14 pagesNitrous Oxide and The Inhalation AnestheticsWiramas Ikhsan Gafar100% (1)
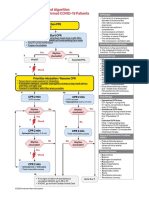
- AlgorithmPALS CACOVID 200406 PDFDocument1 pageAlgorithmPALS CACOVID 200406 PDFEka RahmanizarNo ratings yet
- Delayed Recovery After AnaesthesiaDocument5 pagesDelayed Recovery After Anaesthesiakoolstarone100% (1)
- Inhalation AnestheticsDocument28 pagesInhalation AnestheticsAttaufiq Irawan100% (1)
- Inhalation AnestheticsDocument28 pagesInhalation AnestheticsAttaufiq IrawanNo ratings yet
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- Weight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Document1 pageWeight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Malisa LukmanNo ratings yet
- Inhalation anesthetic agents- Clinical effects and uses - UpToDateDocument65 pagesInhalation anesthetic agents- Clinical effects and uses - UpToDateMedicina DocumentosNo ratings yet
- Pharmacology of General AnesthesiaDocument29 pagesPharmacology of General AnesthesiaNogra CarlNo ratings yet
- Ideal Inhaled Anesthetic Agent CharacteristicsDocument5 pagesIdeal Inhaled Anesthetic Agent CharacteristicsNorjetalexis CabreraNo ratings yet
- General Anaesthetic Agents: Dr. Jacqueline E. CampbellDocument43 pagesGeneral Anaesthetic Agents: Dr. Jacqueline E. CampbellJonathan DavisNo ratings yet
- Clinical Pharmacology For Anesthesiology 2015-320609299 PDFDocument681 pagesClinical Pharmacology For Anesthesiology 2015-320609299 PDFLil_QuinceNo ratings yet
- Anestesia InhaladaDocument6 pagesAnestesia InhaladaHAAGNo ratings yet
- Pharacokinatits and Pharma Co DynamicsDocument18 pagesPharacokinatits and Pharma Co DynamicsPrasad PoluNo ratings yet
- Respon Stres Selama GADocument5 pagesRespon Stres Selama GAAndini Senja AndiraNo ratings yet
- Uptake and Distribution of Volatile AnestheticsDocument22 pagesUptake and Distribution of Volatile AnestheticsSuresh Kumar100% (3)
- 8a. General AnaesthesiaDocument28 pages8a. General Anaesthesiamatchees-gone rogueNo ratings yet
- Maintenance of General Anesthesia - OverviewDocument50 pagesMaintenance of General Anesthesia - Overviewmayteveronica1000No ratings yet
- Understanding General AnestheticsDocument21 pagesUnderstanding General AnestheticsMalueth AnguiNo ratings yet
- Anderson - Total Intravenous Anaesthesia (TIVA) IIDocument4 pagesAnderson - Total Intravenous Anaesthesia (TIVA) IIhlouis8No ratings yet
- Anaesthesia & Intensive Care Medicine Volume 14 Issue 3 2013 (Doi 10.1016/j.mpaic.2013.01.006) Hawthorne, Christopher Sutcliffe, Nick - Total Intravenous Anaesthesia PDFDocument3 pagesAnaesthesia & Intensive Care Medicine Volume 14 Issue 3 2013 (Doi 10.1016/j.mpaic.2013.01.006) Hawthorne, Christopher Sutcliffe, Nick - Total Intravenous Anaesthesia PDFAnonymous nbU88FeNo ratings yet
- An Updated "Norepinephrine Equivalent" Score in Intensive Care As A Marker of Shock SeverityDocument7 pagesAn Updated "Norepinephrine Equivalent" Score in Intensive Care As A Marker of Shock SeveritywenyyyNo ratings yet
- Unlock-Induction ANSE10 WMDocument8 pagesUnlock-Induction ANSE10 WMAl MuzakkiNo ratings yet
- Dose Response Relations Assignment PhysiologyDocument5 pagesDose Response Relations Assignment PhysiologyitsybitsyNo ratings yet
- Jurnal EBCRDocument13 pagesJurnal EBCRDestry AryantyNo ratings yet
- Pharmacology of Inhalational Anaesthetic DrugsDocument6 pagesPharmacology of Inhalational Anaesthetic DrugsAnonymous pJfAvlNo ratings yet
- EpinephrineDocument5 pagesEpinephrinesheynnaNo ratings yet
- Equivalentes NorepinefrinaDocument7 pagesEquivalentes NorepinefrinaHames SeguraNo ratings yet
- General Anesthetics Power PointDocument24 pagesGeneral Anesthetics Power Pointajith9895No ratings yet
- General Anesthetics: Amber JohnsonDocument24 pagesGeneral Anesthetics: Amber JohnsonRamling PatrakarNo ratings yet
- Inhalation Anaesthetic AgentsDocument9 pagesInhalation Anaesthetic Agentsapi-142637023No ratings yet
- Medicine Lecture One General Anaethsia 19th NovDocument102 pagesMedicine Lecture One General Anaethsia 19th NovIrene Zae MwandotoNo ratings yet
- Clinical Pharmacokinetics and PharmacodynamicsDocument20 pagesClinical Pharmacokinetics and PharmacodynamicsAndre MouraNo ratings yet
- Maintenance of General Anesthesia: Overview - UpToDateDocument53 pagesMaintenance of General Anesthesia: Overview - UpToDateEduardoNo ratings yet
- AaaaaDocument128 pagesAaaaaandres bowenNo ratings yet
- Anaesthesia & Intensive Care Medicine Volume 11 Issue 4 2010 (Doi 10.1016/j.mpaic.2009.12.013) Ben Shelley Nick Sutcliffe - Total Intravenous AnaesthesiaDocument3 pagesAnaesthesia & Intensive Care Medicine Volume 11 Issue 4 2010 (Doi 10.1016/j.mpaic.2009.12.013) Ben Shelley Nick Sutcliffe - Total Intravenous AnaesthesiamikhatiarNo ratings yet
- Anesthetic AgentsDocument57 pagesAnesthetic AgentsJustinNo ratings yet
- PHC461 - Principles of Pharmacology CBL2Document12 pagesPHC461 - Principles of Pharmacology CBL2beyonduckNo ratings yet
- Module 4Document18 pagesModule 4nishanth nishanthNo ratings yet
- University of Szeged Pharmacology OutlineDocument24 pagesUniversity of Szeged Pharmacology Outlineola omerNo ratings yet
- Comparative Tolerability Profiles of The Newer Versus Older AntidepressantsDocument29 pagesComparative Tolerability Profiles of The Newer Versus Older AntidepressantsJucas EscobarNo ratings yet
- Hyperbaric Oxygen in Chronic Traumatic Brain Injury: Oxygen, Pressure, and Gene TherapyDocument4 pagesHyperbaric Oxygen in Chronic Traumatic Brain Injury: Oxygen, Pressure, and Gene TherapyAndry SoekamtieNo ratings yet
- Hyperbaric Oxygen in Chronic Traumatic Brain Injury: Oxygen, Pressure, and Gene TherapyDocument4 pagesHyperbaric Oxygen in Chronic Traumatic Brain Injury: Oxygen, Pressure, and Gene TherapyDinNo ratings yet
- 1 s2.0 S2590093521000370 MainDocument9 pages1 s2.0 S2590093521000370 MainIvonne Mercedes Gutierrez AtapaucarNo ratings yet
- Airway Pharmacology: Anesthesia KeyDocument19 pagesAirway Pharmacology: Anesthesia KeyChrispin FaithNo ratings yet
- Acetaminofen y AinesDocument21 pagesAcetaminofen y AinesNadia PMNo ratings yet
- Goulet 1992Document6 pagesGoulet 1992DANIEL - PRISMANo ratings yet
- Bailey 2002Document7 pagesBailey 2002Ayelen GaldeanoNo ratings yet
- Beneficial Effects of Ozone Therapy On Oxidative Stress, Cardiac Functions and Clinical Findings in Patients With Heart Failure Reduced Ejection FractionDocument8 pagesBeneficial Effects of Ozone Therapy On Oxidative Stress, Cardiac Functions and Clinical Findings in Patients With Heart Failure Reduced Ejection FractionCarlosAlbertoCoutinhoNo ratings yet
- General AnaestheticsDocument39 pagesGeneral AnaestheticsImruj LaskarNo ratings yet
- General Anesthetics Effects GuideDocument15 pagesGeneral Anesthetics Effects GuideNikki Tuazon BartolomeNo ratings yet
- Inhalational AnesthesiaDocument96 pagesInhalational AnesthesiaNachee PatricioNo ratings yet
- PK-PD principles for intravenous anestheticsDocument23 pagesPK-PD principles for intravenous anestheticsJonny Bautista AguilarNo ratings yet
- Inhaled Anesthetics IIDocument21 pagesInhaled Anesthetics IIRyan FornollesNo ratings yet
- General Anesthesia 1 PDFDocument49 pagesGeneral Anesthesia 1 PDFYokita JanarthananNo ratings yet
- Anestesicos Locales y La Respuesta InflamatoriaDocument18 pagesAnestesicos Locales y La Respuesta InflamatoriarichabertNo ratings yet
- Pharma Outline - AnestheticsDocument12 pagesPharma Outline - AnestheticsEmmanuel MargateNo ratings yet
- General Anesthesia: Intravenous Induction Agents - UpToDateDocument47 pagesGeneral Anesthesia: Intravenous Induction Agents - UpToDateAhmet PinarbasiNo ratings yet
- The Untoward Effects of Drugs - A Pharmacological and Clinical ManualFrom EverandThe Untoward Effects of Drugs - A Pharmacological and Clinical ManualNo ratings yet
- Maintain CVP ≥8 mm Hg in Septic ShockDocument6 pagesMaintain CVP ≥8 mm Hg in Septic ShockIbrahim DharmawanNo ratings yet
- Abstrak Anu Lampung Revisi FinalDocument1 pageAbstrak Anu Lampung Revisi FinalNisa UcilNo ratings yet
- HSR - USCOM FinalDocument49 pagesHSR - USCOM FinalNisa UcilNo ratings yet
- Perinatology Journal Reading by AhimsaDocument31 pagesPerinatology Journal Reading by AhimsaNisa UcilNo ratings yet
- Airway Management Complications in Children With Difficult Tracheal Intubation From The Pediatric Difficult Intubation PeDI Registry A Prospective Cohort AnalysisDocument10 pagesAirway Management Complications in Children With Difficult Tracheal Intubation From The Pediatric Difficult Intubation PeDI Registry A Prospective Cohort AnalysisNisa UcilNo ratings yet
- Airway Management Complications in Children With Difficult Tracheal Intubation From The Pediatric Difficult Intubation PeDI Registry A Prospective Cohort AnalysisDocument10 pagesAirway Management Complications in Children With Difficult Tracheal Intubation From The Pediatric Difficult Intubation PeDI Registry A Prospective Cohort AnalysisNisa UcilNo ratings yet
- Algo Pals BLS Pediatric Cardiac ArrestDocument1 pageAlgo Pals BLS Pediatric Cardiac ArrestSiti NabilaNo ratings yet
- Exercise During Pregnancy A Practical ApproachDocument7 pagesExercise During Pregnancy A Practical ApproachNisa UcilNo ratings yet
- NeurologicDocument7 pagesNeurologicFarrah ErmanNo ratings yet
- Carrot, Angel and Oreo cake recipesDocument4 pagesCarrot, Angel and Oreo cake recipesNisa UcilNo ratings yet
- Algo Pals Pediatric BradycardiaDocument1 pageAlgo Pals Pediatric BradycardiaNisa UcilNo ratings yet
- Infantile Pityriasis Alba and Comorbid DisordersDocument5 pagesInfantile Pityriasis Alba and Comorbid DisordersNisa UcilNo ratings yet
- Nihms 701642Document10 pagesNihms 701642Nisa UcilNo ratings yet
- The Prevalence of Interatrial Septal Openings in Newborns and Predictive Factors For Spontaneous ClosureDocument5 pagesThe Prevalence of Interatrial Septal Openings in Newborns and Predictive Factors For Spontaneous ClosureNisa UcilNo ratings yet
- Algo Pals Pediatric Cardiac ArrestDocument1 pageAlgo Pals Pediatric Cardiac ArrestDevi ChrestellaNo ratings yet
- Review Article: Autoimmune/Inflammatory Arthritis Associated Lymphomas: Who Is at Risk?Document12 pagesReview Article: Autoimmune/Inflammatory Arthritis Associated Lymphomas: Who Is at Risk?Nisa UcilNo ratings yet
- Exercise During Pregnancy A Practical ApproachDocument7 pagesExercise During Pregnancy A Practical ApproachNisa UcilNo ratings yet
- Early detection of autism with CHAT checklistDocument44 pagesEarly detection of autism with CHAT checklistNisa UcilNo ratings yet
- Adverson, J. 2013. Feeding Children With CP Swallowing Difficulties PDFDocument4 pagesAdverson, J. 2013. Feeding Children With CP Swallowing Difficulties PDFNicoleOrtegaAguileraNo ratings yet
- Maternal and Infant Risk Factors Associated with Neonatal Asphyxia in BaliDocument6 pagesMaternal and Infant Risk Factors Associated with Neonatal Asphyxia in BaliNisa UcilNo ratings yet
- Isk AafpDocument7 pagesIsk Aafpbebekdd22No ratings yet
- Cerebrospinal Fluid Lactate and PyruvateDocument8 pagesCerebrospinal Fluid Lactate and PyruvateNisa UcilNo ratings yet
- 66b3 PDFDocument6 pages66b3 PDFNisa UcilNo ratings yet
- Karagol 2010Document4 pagesKaragol 2010Nisa UcilNo ratings yet
- Isk AafpDocument7 pagesIsk Aafpbebekdd22No ratings yet
- Correlation of Procalcitonin Level and Neutrophil-Lymphocyte Ratio in SIRS PatientsDocument1 pageCorrelation of Procalcitonin Level and Neutrophil-Lymphocyte Ratio in SIRS PatientsNisa UcilNo ratings yet
- PCH 32 s1 039 PDFDocument4 pagesPCH 32 s1 039 PDF79lalalaNo ratings yet
- Validity and ReliabilityDocument6 pagesValidity and ReliabilityfarlynzNo ratings yet