You might also like
- 7.0 Skeletal SystemDocument45 pages7.0 Skeletal System[R2A] Khadijah Azlan100% (1)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Anatomy 1.02 Axial SkeletonDocument8 pagesAnatomy 1.02 Axial SkeletonMark AbrazaldoNo ratings yet
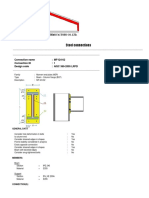
- Steel Connections: Connection Name: MF-I24-02 Connection ID: 1 Design Code: AISC 360-2005 LRFDDocument12 pagesSteel Connections: Connection Name: MF-I24-02 Connection ID: 1 Design Code: AISC 360-2005 LRFDmalikasalNo ratings yet
- Structural Calculation For Directly Welded Flange FR Moment Connection (Beam-To-Column Flange)Document10 pagesStructural Calculation For Directly Welded Flange FR Moment Connection (Beam-To-Column Flange)danieldumapitNo ratings yet
- Novenas and PrayersDocument5 pagesNovenas and PrayersDenver TanhuanNo ratings yet
- Novenas and PrayersDocument5 pagesNovenas and PrayersDenver TanhuanNo ratings yet
- Part 1 (Final 2022-11-21)Document28 pagesPart 1 (Final 2022-11-21)saraNo ratings yet
- ISO 3834purchasedocumentDocument8 pagesISO 3834purchasedocumenthector-salomonNo ratings yet
- Introduction To Skeletal 1Document196 pagesIntroduction To Skeletal 1Earl TrinidadNo ratings yet
- Digital Ultrasonic Flaw Detectors For Curved SurfaceDocument11 pagesDigital Ultrasonic Flaw Detectors For Curved Surfaceiprao0% (1)
- Shear Wave PDFDocument6 pagesShear Wave PDFcutefrenzyNo ratings yet
- MCQs in Connective Tissue and BloodDocument7 pagesMCQs in Connective Tissue and Bloodashour_abdelsalam632681% (27)
- Section 2 - Thread - BasicsDocument27 pagesSection 2 - Thread - BasicsChris MedeirosNo ratings yet
- Result Summary - Overall: Moment Connection - Beam Splice Code AISC 360-16 LRFDDocument6 pagesResult Summary - Overall: Moment Connection - Beam Splice Code AISC 360-16 LRFDMichenerparkNo ratings yet
- Engineering DrawingDocument157 pagesEngineering DrawingLab Thermo100% (1)
- Joints and Its ClassificationDocument30 pagesJoints and Its Classificationdeepuphysio100% (10)
- AISC steel connection design documentDocument17 pagesAISC steel connection design documentSh MNNo ratings yet
- Hole's Human Anatomy and Physiology: 5 Skeletal SystemDocument73 pagesHole's Human Anatomy and Physiology: 5 Skeletal SystemLongyapon Sheena StephanieNo ratings yet
- Geometrical TolerancingDocument12 pagesGeometrical TolerancingItalo Venegas100% (1)
- Benchmarking Process ExplainedDocument2 pagesBenchmarking Process ExplainedDenver TanhuanNo ratings yet
- Cell Biology Review: Blood Smear and Connective TissueDocument15 pagesCell Biology Review: Blood Smear and Connective TissueGabriel ParasNo ratings yet
- Ut Job Knowledge - TwiDocument10 pagesUt Job Knowledge - TwiBhanu Pratap ChoudhuryNo ratings yet
- Metrology Lab w2014Document15 pagesMetrology Lab w2014ObaidNo ratings yet
- New Microsoft Office Word DocumentDocument9 pagesNew Microsoft Office Word DocumentKhalid PerwezNo ratings yet
- Chevron ConnectionDocument35 pagesChevron ConnectionAbdelrahman YoussefNo ratings yet
- Musculoskeletal Anatomy and Physiology 4Document67 pagesMusculoskeletal Anatomy and Physiology 4Dennis Nabor Muñoz, RN,RM100% (1)
- Fab 01 QA of Welds, ISO 3834, RWC Etc.Document17 pagesFab 01 QA of Welds, ISO 3834, RWC Etc.Raghu vamshiNo ratings yet
- Lecture Guide Assessment-Of-Musculoskeletal-Function HPDocument85 pagesLecture Guide Assessment-Of-Musculoskeletal-Function HPBlessed GarcianoNo ratings yet
- ALVEOLAR BoneDocument72 pagesALVEOLAR BoneArchana50% (2)
- Cswip 3.1 2011Document400 pagesCswip 3.1 2011Anonymous SA40GK6No ratings yet
- Standard And/or Project Stage TC: Filter The ListDocument10 pagesStandard And/or Project Stage TC: Filter The ListIsmailNo ratings yet
- Bone TissueDocument66 pagesBone TissueFunikawati Baldiyah100% (1)
- Weldability Test For Thin Sheet MaterialsDocument6 pagesWeldability Test For Thin Sheet MaterialsAnonymous FHkX0ANo ratings yet
- RossDocument436 pagesRossAna Ion100% (1)
- Module 3 Construction and DesignDocument5 pagesModule 3 Construction and DesignDhimas Surya Negara100% (1)
- WELD DESIGN CHECK FOR ANCHOR SUPPORTDocument8 pagesWELD DESIGN CHECK FOR ANCHOR SUPPORTUmer AziqNo ratings yet
- Simboluri SudareDocument8 pagesSimboluri SudarecornelutsNo ratings yet
- Hardness TestDocument25 pagesHardness TestDeniThomasBoban100% (1)
- Osteoarthritis Case StudyDocument29 pagesOsteoarthritis Case StudyColeen Mae CamaristaNo ratings yet
- Quality Inspection - WeldingDocument4 pagesQuality Inspection - WeldingMin Min Mit100% (1)
- Chapter 6 Bone Tissue 2304Document37 pagesChapter 6 Bone Tissue 2304Sav Oli100% (1)
- Basic Review CardDocument6 pagesBasic Review CardSheena LeavittNo ratings yet
- Deformity Around KneeDocument94 pagesDeformity Around KneeVarun Vijay100% (3)
- GVO 03 Anatomy EN PDFDocument84 pagesGVO 03 Anatomy EN PDFAlexandre FunciaNo ratings yet
- Engg - Drawing 1st Year LMDocument167 pagesEngg - Drawing 1st Year LMPRIYABRATA JENANo ratings yet
- AISC Properties MM GPP 2017Document87 pagesAISC Properties MM GPP 2017Pablo García PeñaNo ratings yet
- AWS Catalog 2017 Winter SpringDocument52 pagesAWS Catalog 2017 Winter SpringPilar Medrano MenaNo ratings yet
- AWS Weld Symbol BasicsDocument3 pagesAWS Weld Symbol Basicschairul anwarNo ratings yet
- Science Olympiad 2020 Cheat SheetDocument4 pagesScience Olympiad 2020 Cheat SheetLisa RetbergNo ratings yet
- Engineering Drawing Notes BDocument50 pagesEngineering Drawing Notes BsrchougulaNo ratings yet
- Introduction To Non-Destructive TestingDocument34 pagesIntroduction To Non-Destructive Testingegy pure100% (1)
- How To Read Welding GaugesDocument8 pagesHow To Read Welding GaugeshemnNo ratings yet
- Welder Qualification Test Log: Engineering Standards Manual OST220-03-01-ESM Chapter 13, WeldingDocument1 pageWelder Qualification Test Log: Engineering Standards Manual OST220-03-01-ESM Chapter 13, WeldingReza100% (1)
- Measuring Fillet Weld Size It's Easy Right - Karsten Madsen - Pulse - LinkedInDocument5 pagesMeasuring Fillet Weld Size It's Easy Right - Karsten Madsen - Pulse - LinkedInnkvonNo ratings yet
- A Review of The Application of Weld Symbols On Drawings - Part 2 - Job Knowledge 65Document5 pagesA Review of The Application of Weld Symbols On Drawings - Part 2 - Job Knowledge 65tuanNo ratings yet
- Discovering Welding PolarityDocument2 pagesDiscovering Welding PolarityShafiq AhmadNo ratings yet
- Miller - 2010 Welding Heavy Structural Steel SucessfulyyDocument15 pagesMiller - 2010 Welding Heavy Structural Steel SucessfulyyLleiLleiNo ratings yet
- Welding Terms & Definitions GuideDocument108 pagesWelding Terms & Definitions Guidearland_limNo ratings yet
- Applicable ASTM Specifications For Structural Fasteners: Table 3.8 Anchor RodsDocument1 pageApplicable ASTM Specifications For Structural Fasteners: Table 3.8 Anchor Rodsivan bolañosNo ratings yet
- Cswip 3.1 QuizDocument70 pagesCswip 3.1 Quizalzaki100% (1)
- EW 512 6 Nondestructive TestingDocument37 pagesEW 512 6 Nondestructive TestingHarun HodžićNo ratings yet
- Module 4 Weld Geometry and Welding Symbols-1Document87 pagesModule 4 Weld Geometry and Welding Symbols-1Miki JaksicNo ratings yet
- Electron Beam Welding-Manu AssignmentDocument5 pagesElectron Beam Welding-Manu Assignmentbaiti_atiqahNo ratings yet
- Gen - Importance of Welding in L & T PDFDocument30 pagesGen - Importance of Welding in L & T PDFSivaNo ratings yet
- Bone TissueDocument66 pagesBone TissueWalter Macasiano GravadorNo ratings yet
- Histology of A BoneDocument26 pagesHistology of A BoneAmanuel MaruNo ratings yet
- Musculoskeletal System-Topic 8Document40 pagesMusculoskeletal System-Topic 8Heba TabchNo ratings yet
- Dr. Sassia Lecture Bone Histology Part I June 2023Document45 pagesDr. Sassia Lecture Bone Histology Part I June 2023Ali ELKARGHALYNo ratings yet
- Biol 111-Bones and Skeletal Tissue Part 1Document58 pagesBiol 111-Bones and Skeletal Tissue Part 1Jaedon AdamsNo ratings yet
- Skeletal - System AnatomyDocument130 pagesSkeletal - System Anatomyhamnafaisall8No ratings yet
- Overview of The Musculoskeletal System: For Year 1 Medicine By: Zelalem.aDocument36 pagesOverview of The Musculoskeletal System: For Year 1 Medicine By: Zelalem.aAmanuel MaruNo ratings yet
- Impact of Typhoon Ulysses on Community Health and Livelihood in Quezon ProvinceDocument1 pageImpact of Typhoon Ulysses on Community Health and Livelihood in Quezon ProvinceDenver Tanhuan100% (1)
- 4 Fundamental Elements of Company Analysis: Valuation, Quality, Growth & StatsDocument1 page4 Fundamental Elements of Company Analysis: Valuation, Quality, Growth & StatsDenver TanhuanNo ratings yet
- 17 08 PDFDocument1 page17 08 PDFDenver TanhuanNo ratings yet
- FIL Stock MarketDocument41 pagesFIL Stock Marketrekha_kumariNo ratings yet
- 4 Fundamental Elements of Company Analysis: Valuation, Quality, Growth & StatsDocument1 page4 Fundamental Elements of Company Analysis: Valuation, Quality, Growth & StatsDenver TanhuanNo ratings yet
- 4 Fundamental Elements of Company Analysis: Valuation, Quality, Growth & StatsDocument1 page4 Fundamental Elements of Company Analysis: Valuation, Quality, Growth & StatsDenver TanhuanNo ratings yet
- FIL Stock MarketDocument41 pagesFIL Stock Marketrekha_kumariNo ratings yet
- RR 12-2013Document1 pageRR 12-2013Denver TanhuanNo ratings yet
- Conduct CIS Audit GuideDocument1 pageConduct CIS Audit GuideDenver TanhuanNo ratings yet
- BiospyDocument2 pagesBiospyDenver TanhuanNo ratings yet
- ADocument1 pageADenver TanhuanNo ratings yet
- Lease Bonus Paidby The Lessee Treatment)Document2 pagesLease Bonus Paidby The Lessee Treatment)Denver TanhuanNo ratings yet
- MedicineDocument1 pageMedicineDenver TanhuanNo ratings yet
- Pathophysiology of OsteoarthritisDocument3 pagesPathophysiology of OsteoarthritisHajar ToharNo ratings yet
- Penyakit Sendi Degeneratif & Patologi TulangDocument38 pagesPenyakit Sendi Degeneratif & Patologi TulangSaddam ZakariyaNo ratings yet
- Diffusion and ReactionDocument54 pagesDiffusion and ReactionAfrica Meryll100% (1)
- Musculoskeletal System Assessment: - OverviewDocument5 pagesMusculoskeletal System Assessment: - OverviewDenise BarayogaNo ratings yet
- BIO2OO - Introduction Tissues, Classification of Living Things & Ecology 1.1.0 Animal TissueDocument19 pagesBIO2OO - Introduction Tissues, Classification of Living Things & Ecology 1.1.0 Animal TissueMark SullivanNo ratings yet
- Homework 6 - JointsDocument5 pagesHomework 6 - JointsAdwoa OkohNo ratings yet
- MUSKULOSKELETAL Supplemental SlidesDocument180 pagesMUSKULOSKELETAL Supplemental Slidesstuffednurse100% (1)
- 6 JointDocument11 pages6 Jointيزن الحارثيNo ratings yet
- Primary Human Chondrocytes and Chondrocyte Growth MediaDocument4 pagesPrimary Human Chondrocytes and Chondrocyte Growth Mediablack0229No ratings yet
- Pathology of OsteoarthritisDocument2 pagesPathology of OsteoarthritisYogi drNo ratings yet
- Structure and Function of The Skeletal System: Skeleton Dried Up BodyDocument4 pagesStructure and Function of The Skeletal System: Skeleton Dried Up BodyKenn yahweexNo ratings yet
- Chapter 4, Tissues, Part 2: Histology The Study of Tissues Tissue A Collection of Cells That Perform RelatedDocument31 pagesChapter 4, Tissues, Part 2: Histology The Study of Tissues Tissue A Collection of Cells That Perform RelatedSajid NadafNo ratings yet
- Artlife India Joint Care Products for Musculoskeletal SystemDocument5 pagesArtlife India Joint Care Products for Musculoskeletal SystemCelly MarshalNo ratings yet
- Week 4: Bones and Cartilage Quiz - Lecture: Attempt HistoryDocument9 pagesWeek 4: Bones and Cartilage Quiz - Lecture: Attempt HistoryZyrea HarwoleNo ratings yet
- OrthopaedicsDocument3 pagesOrthopaedicsnicewanNo ratings yet
- Histo 1st ShiftDocument25 pagesHisto 1st ShiftIvy CruzNo ratings yet
- المحاضرة الثانية تشريح اسنان م 1Document26 pagesالمحاضرة الثانية تشريح اسنان م 1mfhrluvxxxNo ratings yet
- Lesson 2 Skeletal SystemDocument79 pagesLesson 2 Skeletal SystemLemuel CunananNo ratings yet
- 1 The Development and Growth of The FaceDocument15 pages1 The Development and Growth of The FacebarbiemeNo ratings yet
- Diffusion and ReactionDocument54 pagesDiffusion and ReactionRambabu PonnalaNo ratings yet
- Effects of Aging and Physical Activity On Articular Cartilage-A Literature ReviewDocument7 pagesEffects of Aging and Physical Activity On Articular Cartilage-A Literature ReviewAlcii PereiraNo ratings yet
- Chapter 11 - Skeletal System Morphophys - 2020 - The Zebrafish in Biomedical ResDocument6 pagesChapter 11 - Skeletal System Morphophys - 2020 - The Zebrafish in Biomedical ResNicolas BaronNo ratings yet