You might also like
- Basics of Neonatal Ventilation 1Document42 pagesBasics of Neonatal Ventilation 1Abid Ali Rizvi100% (1)
- Neonatal Ventilation PDFDocument29 pagesNeonatal Ventilation PDFIsabella HosanaNo ratings yet
- Mechanical Ventilation in Pediatric PracticeDocument11 pagesMechanical Ventilation in Pediatric PracticeHandris YanitraNo ratings yet
- Neonatal Ventilation, First StepDocument101 pagesNeonatal Ventilation, First StepJimena JuarezNo ratings yet
- Neonatal Ventilation - Basics of Mechanical Ventilation: Authors: Sam Wallis - Catriona FirthDocument21 pagesNeonatal Ventilation - Basics of Mechanical Ventilation: Authors: Sam Wallis - Catriona FirthEduardo Rios DuboisNo ratings yet
- Mechanical Ventilation in NeonatesDocument60 pagesMechanical Ventilation in NeonatesZuhair Aldajani زهير عمر الدجاني100% (3)
- Neonatal Ventilation - Neocon 2017-2Document156 pagesNeonatal Ventilation - Neocon 2017-2RAM SOFTWARE100% (2)
- Newborn Care Hnadbook by 2019 ClassDocument267 pagesNewborn Care Hnadbook by 2019 Classknowledge chanall chanallNo ratings yet
- Nicu Must KnowsDocument7 pagesNicu Must KnowsCyfern100% (2)
- Step by Step Neonatal Ventilation PDFDocument99 pagesStep by Step Neonatal Ventilation PDFUtuh Kalambuai50% (2)
- NRP Exam InstructionsDocument2 pagesNRP Exam InstructionsjermumNo ratings yet
- A Guide To The Newborn Intensive Care Unit (NICU)Document36 pagesA Guide To The Newborn Intensive Care Unit (NICU)Jean Wallace100% (3)
- Neonatal EmergenciesDocument123 pagesNeonatal EmergenciesMaria Babette Almazan Talavera100% (2)
- Neonatal Ventilation Made EasyDocument97 pagesNeonatal Ventilation Made EasyCảnh HoàngNo ratings yet
- NICU Pocket GuideDocument28 pagesNICU Pocket GuideCharles S. Williams RRT, AE-C86% (7)
- HFOV High-Frequency-Oscillatory-VentilationDocument22 pagesHFOV High-Frequency-Oscillatory-VentilationJZNo ratings yet
- Interpretting Neonatal Xrays (Click Enable Macros)Document304 pagesInterpretting Neonatal Xrays (Click Enable Macros)John Phamnguyen100% (5)
- Pediatric Mechanical VentilationDocument49 pagesPediatric Mechanical VentilationNirubhana ArunthavasothyNo ratings yet
- Neonatal Resuscitation Program: 7 EditionDocument64 pagesNeonatal Resuscitation Program: 7 EditionStacy LuceroNo ratings yet
- Neonatal Golden HourDocument28 pagesNeonatal Golden HourGendis Ayu ArdiasNo ratings yet
- NICU ProtocolDocument75 pagesNICU ProtocolCatherine Lee100% (6)
- Pediatric and Neonatal Respiratory Care PDFDocument608 pagesPediatric and Neonatal Respiratory Care PDFekaNo ratings yet
- Neonatal ResuscitationDocument7 pagesNeonatal Resuscitation2012100% (3)
- Pediatric and Neonatal Mecanical Ventilation PDFDocument309 pagesPediatric and Neonatal Mecanical Ventilation PDFsdufhq100% (1)
- Neonatal Care Protocols for Hospital PhysiciansDocument648 pagesNeonatal Care Protocols for Hospital PhysiciansИван Мельник100% (1)
- Neonatal Ventilator Vent Set-Up CheatsheetDocument1 pageNeonatal Ventilator Vent Set-Up CheatsheetRick Frea50% (2)
- Neonatal Resuscitation Program Quick Equipment Checklist-NRP 6THDocument7 pagesNeonatal Resuscitation Program Quick Equipment Checklist-NRP 6THdrtgodeNo ratings yet
- American Academy of PediatricsDocument320 pagesAmerican Academy of PediatricsJuan Sebasatián Arjona100% (2)
- Non Invasive Ventilation in PediatricsDocument192 pagesNon Invasive Ventilation in Pediatricstj1983tj0% (1)
- Guidelines For Use of Bubble-CPAP ConcentratorsDocument10 pagesGuidelines For Use of Bubble-CPAP ConcentratorsevanNo ratings yet
- NMCSD Nicu 2015Document39 pagesNMCSD Nicu 2015Bibu BhaskarNo ratings yet
- Neonatal Reurscitation PDFDocument347 pagesNeonatal Reurscitation PDFAlina Andreica100% (1)
- NICU Orientation ManualDocument27 pagesNICU Orientation Manualsedaka26100% (1)
- NRP 2011 SummaryDocument6 pagesNRP 2011 Summaryvanstar7No ratings yet
- Stable 2Document115 pagesStable 2Avyel KramNo ratings yet
- SrableDocument39 pagesSrableYatza Sanches SanchesNo ratings yet
- Ventilator Graphics PDFDocument30 pagesVentilator Graphics PDFRina AnggrainiNo ratings yet
- Nursing the NeonateFrom EverandNursing the NeonateMaggie MeeksNo ratings yet
- IV Fluid Guidelines for Kids and NewbornsDocument16 pagesIV Fluid Guidelines for Kids and NewbornsWidyadarya Triyono PutriNo ratings yet
- NICU Manual Cheat SheetDocument2 pagesNICU Manual Cheat Sheetlori_quintal92% (13)
- Non Invasive Ventilation Techniques for Respiratory DistressDocument76 pagesNon Invasive Ventilation Techniques for Respiratory DistressTitik sukamtiNo ratings yet
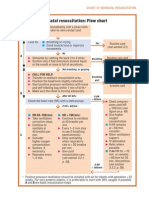
- Neonatal Resuscitation Program Flow ChartDocument3 pagesNeonatal Resuscitation Program Flow ChartChin Nam80% (5)
- Care of Normal Newborn BabiesDocument439 pagesCare of Normal Newborn BabiesSebastian Spatariu100% (2)
- Essentials of Pediatric Emergency MedicineFrom EverandEssentials of Pediatric Emergency MedicineRating: 4.5 out of 5 stars4.5/5 (3)
- Nicu Survival Guide For ResidentsDocument26 pagesNicu Survival Guide For ResidentspeppepagNo ratings yet
- Persistent Pulmonary Hypertension in Newborn: By: Dr. Abhay Kumar Moderator: Dr. Akhilesh KumarDocument31 pagesPersistent Pulmonary Hypertension in Newborn: By: Dr. Abhay Kumar Moderator: Dr. Akhilesh KumarAbhay BarnwalNo ratings yet
- The Blood Transfusion Protocol. LatestDocument38 pagesThe Blood Transfusion Protocol. Latestdarshan drNo ratings yet
- Evidence Based Guidelines For Prevention of Infection in NicuDocument50 pagesEvidence Based Guidelines For Prevention of Infection in NicuBahaa Gamal100% (2)
- Sepsis Neonatal: Bryan L Ohning, MD, PHD, Clinical Associate Professor of Pediatrics, MedicalDocument43 pagesSepsis Neonatal: Bryan L Ohning, MD, PHD, Clinical Associate Professor of Pediatrics, Medicalapi-19492580No ratings yet
- CPAPDocument53 pagesCPAPvibhurocksNo ratings yet
- NEONATAL NURSE PRACTITIONER: Passbooks Study GuideFrom EverandNEONATAL NURSE PRACTITIONER: Passbooks Study GuideNo ratings yet
- Pediatric Potpourri 200+ New CPEN Questions: Certified Pediatric Emergency Nurse Review (3rd Edition Supplement)From EverandPediatric Potpourri 200+ New CPEN Questions: Certified Pediatric Emergency Nurse Review (3rd Edition Supplement)No ratings yet
- NEONATAL INTENSIVE CARE NURSING: Passbooks Study GuideFrom EverandNEONATAL INTENSIVE CARE NURSING: Passbooks Study GuideNo ratings yet
- Pediatric Cardiology and Pulmonology: A Practically Painless ReviewFrom EverandPediatric Cardiology and Pulmonology: A Practically Painless ReviewNo ratings yet
- Neonatal Respiratory DistressFrom EverandNeonatal Respiratory DistressPhilip M FarrellRating: 5 out of 5 stars5/5 (1)
- Neonatal Nurse Practitioner A Complete Guide - 2020 EditionFrom EverandNeonatal Nurse Practitioner A Complete Guide - 2020 EditionNo ratings yet
- Fetal and Neonatal DisordersFrom EverandFetal and Neonatal DisordersNicholas S. AssaliNo ratings yet
- LOW RISK NEONATAL NURSING: Passbooks Study GuideFrom EverandLOW RISK NEONATAL NURSING: Passbooks Study GuideNo ratings yet
- Drager - Evita2 - enDocument141 pagesDrager - Evita2 - enGabriel JanuárioNo ratings yet
- Respiratory Treatments For COVID-19 SOP - Updated Feb. 2021Document2 pagesRespiratory Treatments For COVID-19 SOP - Updated Feb. 2021Abhishek GoelNo ratings yet
- Introducing Radiology SolutionsDocument60 pagesIntroducing Radiology Solutionserc001No ratings yet
- Trends and Issues in Nursing (CPD)Document13 pagesTrends and Issues in Nursing (CPD)Maizatul Akmar IbrahimNo ratings yet
- RSP New Nomenclature Ventilation Modes Icu Booklet 9066477 enDocument72 pagesRSP New Nomenclature Ventilation Modes Icu Booklet 9066477 enNasro Juv100% (1)
- Ventilation Systems and AccessoriesDocument3 pagesVentilation Systems and Accessoriesjuan alberto florez coteNo ratings yet
- Ayurveda Dispensaries Listing in GujaratDocument18 pagesAyurveda Dispensaries Listing in GujaratDipesh PatelNo ratings yet
- Dental Radiography Principles and Techniques 4th Edition Iannucci Test BankDocument25 pagesDental Radiography Principles and Techniques 4th Edition Iannucci Test BankVanessaCurtisfcrxn100% (59)
- Prospectus of Paramedical College in Delhi - IPHIDocument16 pagesProspectus of Paramedical College in Delhi - IPHIParamedical CollegeinDelhiNo ratings yet
- The Journey of Radiology in EthiopiaDocument8 pagesThe Journey of Radiology in EthiopiaAnonymous 9dVZCnTXSNo ratings yet
- DR Anne Webster Maiden SpeechDocument17 pagesDR Anne Webster Maiden SpeechAlexander DarlingNo ratings yet
- Panchakarma in Netra RogaDocument27 pagesPanchakarma in Netra RogaAnanthram Sharma86% (7)
- Final Resume PDFDocument4 pagesFinal Resume PDFapi-498720485No ratings yet
- Screenshot 2021-05-20 at 16.38.32Document14 pagesScreenshot 2021-05-20 at 16.38.32refqi adhyaksNo ratings yet
- Balance Comprobacion Mensualizado Diciembre 2022Document65 pagesBalance Comprobacion Mensualizado Diciembre 2022Milagros ObregonNo ratings yet
- APPS 2013 Japan WorkshopDocument19 pagesAPPS 2013 Japan WorkshopExaudi EbennezerNo ratings yet
- CT Radiation Dose and Radiation Reduction Strategies: Focused Issue of This MonthDocument7 pagesCT Radiation Dose and Radiation Reduction Strategies: Focused Issue of This MonthHarley Alejo MNo ratings yet
- Healthcare Service in Hong Kong and Its Challenges: China PerspectivesDocument9 pagesHealthcare Service in Hong Kong and Its Challenges: China PerspectivesGrace LNo ratings yet
- Varian Single Energy Linear AcceleratorsDocument26 pagesVarian Single Energy Linear AcceleratorsHerman HalimNo ratings yet
- Test Bank For Merrills Atlas of Radiographic Positioning and Procedures 13th Edition by LongDocument6 pagesTest Bank For Merrills Atlas of Radiographic Positioning and Procedures 13th Edition by Longdominicmaximus44uNo ratings yet
- Health Grade10 4th QuarterDocument40 pagesHealth Grade10 4th Quarterd-fbuser-33831503179% (185)
- Understanding Mechanical Ventilation Modes & WeaningDocument52 pagesUnderstanding Mechanical Ventilation Modes & WeaningDeepa BhattacharjeeNo ratings yet
- Kel 1 - Hospital Jobs and Personnel, Hospital Departments and Facilities - 20231026 - 192042 - 0000Document37 pagesKel 1 - Hospital Jobs and Personnel, Hospital Departments and Facilities - 20231026 - 192042 - 0000Jhean FirtsaNo ratings yet
- SoalDocument4 pagesSoalWulandhariNo ratings yet
- High-Flow Nasal Cannula Pada Anak (Literatur Review) : Avalilable OnlineDocument12 pagesHigh-Flow Nasal Cannula Pada Anak (Literatur Review) : Avalilable Onlinejeinzen14No ratings yet
- Tarif Layanan Rssa 2018 FixDocument49 pagesTarif Layanan Rssa 2018 FixRSUD SITI AISYAH100% (1)
- What Is A Career?: Components and Steps in Making A Health Career PlanDocument9 pagesWhat Is A Career?: Components and Steps in Making A Health Career PlanDaphne CuaresmaNo ratings yet
- Question: Methods of Radiology Imaging.: Assignment 01 Muskaan FatimaDocument4 pagesQuestion: Methods of Radiology Imaging.: Assignment 01 Muskaan FatimaMuskan FatimaNo ratings yet
- Mechanical Ventilation: Settings and Basic Modes: Term Clinical Considerations Fraction of Inspired Oxygen (Fio)Document5 pagesMechanical Ventilation: Settings and Basic Modes: Term Clinical Considerations Fraction of Inspired Oxygen (Fio)Luis LopezNo ratings yet
- Bariño, Patricia Jamin: Online Grades InquiryDocument1 pageBariño, Patricia Jamin: Online Grades InquirySamiracomputerstation Kuya MarvsNo ratings yet