You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Modified Quad HelixDocument5 pagesModified Quad HelixFirma Nurdinia DewiNo ratings yet
- 3Mix-MP in Endodontics - An overview of the triple antibiotic pasteDocument10 pages3Mix-MP in Endodontics - An overview of the triple antibiotic pasteFirma Nurdinia DewiNo ratings yet
- Critical and Unexpected Findings Reporting Policy 1Document8 pagesCritical and Unexpected Findings Reporting Policy 1Firma Nurdinia DewiNo ratings yet
- A New Modified Tandem Appliance For Management of Developing Class III MalocclusionDocument5 pagesA New Modified Tandem Appliance For Management of Developing Class III MalocclusionFirma Nurdinia DewiNo ratings yet
- Dentinogenesis GigiDocument5 pagesDentinogenesis GigiFirma Nurdinia DewiNo ratings yet
- KonservasiDocument7 pagesKonservasiFirma Nurdinia DewiNo ratings yet
- Compound Compleks OdontomaDocument6 pagesCompound Compleks OdontomaFirma Nurdinia DewiNo ratings yet
- Klas 3 KoreksiDocument8 pagesKlas 3 KoreksiFirma Nurdinia DewiNo ratings yet
- Catlan's ApplianceDocument5 pagesCatlan's ApplianceFirma Nurdinia DewiNo ratings yet
- Dentinogenesis GigiDocument5 pagesDentinogenesis GigiFirma Nurdinia DewiNo ratings yet
- 3 MixDocument8 pages3 MixFirma Nurdinia DewiNo ratings yet
- Non-Surgical Treatment of Periapical Lesion Using Calcium Hydroxide-A Case ReportDocument4 pagesNon-Surgical Treatment of Periapical Lesion Using Calcium Hydroxide-A Case ReportNadya PurwantyNo ratings yet
- Compound Compleks OdontomaDocument6 pagesCompound Compleks OdontomaFirma Nurdinia DewiNo ratings yet
- 3 MixDocument6 pages3 MixFirma Nurdinia DewiNo ratings yet
- 3 MixDocument4 pages3 MixFirma Nurdinia DewiNo ratings yet
- 3mix MPDocument6 pages3mix MPFirma Nurdinia DewiNo ratings yet
- OrthiDocument16 pagesOrthiFirma Nurdinia DewiNo ratings yet
- KonservasiDocument7 pagesKonservasiFirma Nurdinia DewiNo ratings yet
- 1 1 8-25 PDFDocument18 pages1 1 8-25 PDFYunisca SeptianiNo ratings yet
- Periodontal Host Modulation With Antiproteinase Anti Inflammatory and Bone Sparing AgentsDocument26 pagesPeriodontal Host Modulation With Antiproteinase Anti Inflammatory and Bone Sparing AgentsVrushali BhoirNo ratings yet
- 3 MixDocument8 pages3 MixFirma Nurdinia DewiNo ratings yet
- OrthodonticDocument3 pagesOrthodonticFirma Nurdinia DewiNo ratings yet
- v04 n04 01Document17 pagesv04 n04 01Firma Nurdinia DewiNo ratings yet
- Kekambuhan Gingivitis Hiperplasi Setelah Gingivektomi: (Recurrent of Hyperplastic Gingivitis After Gingivectomy)Document4 pagesKekambuhan Gingivitis Hiperplasi Setelah Gingivektomi: (Recurrent of Hyperplastic Gingivitis After Gingivectomy)Firman LongtankNo ratings yet
- Obat KBDocument4 pagesObat KBFirma Nurdinia DewiNo ratings yet
- LeukemiaDocument6 pagesLeukemiaFirma Nurdinia DewiNo ratings yet
- PerokokDocument6 pagesPerokokFirma Nurdinia DewiNo ratings yet
- LeukemiaDocument6 pagesLeukemiaFirma Nurdinia DewiNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Diabetes MellitusDocument48 pagesDiabetes Mellitusladylisette67% (3)
- Anaphy Finals ReviewerDocument193 pagesAnaphy Finals Reviewerxuxi dulNo ratings yet
- Congenital Hypothyroidism: Screening, Diagnosis, Management, and OutcomeDocument7 pagesCongenital Hypothyroidism: Screening, Diagnosis, Management, and OutcomeIbrahim Abdul KareemNo ratings yet
- 12 Liver-FunctionDocument6 pages12 Liver-FunctionSubhi MishraNo ratings yet
- Causes of Endocrine DisordersDocument8 pagesCauses of Endocrine DisordersKrystel Mae GarciaNo ratings yet
- Adrenal hormones: fight or flight responseDocument49 pagesAdrenal hormones: fight or flight responseNona NanoNo ratings yet
- Molecular ClockworkDocument10 pagesMolecular Clockworkgarsa psikiatriNo ratings yet
- Myocardial InfarctionDocument12 pagesMyocardial InfarctionRifka Meilinda Putri IINo ratings yet
- 821566642727unit-2 - Nutrition and DieteticsDocument12 pages821566642727unit-2 - Nutrition and DieteticsGaganpreet Kaur Fashion DesigningNo ratings yet
- 2562 - PDF OmigatDocument11 pages2562 - PDF OmigatkhansarafidaNo ratings yet
- Garret's Personal Diet Plan!: Meal 1Document2 pagesGarret's Personal Diet Plan!: Meal 1garrettNo ratings yet
- Cushing'S Syndrome and Cushing'S Disease: Your Questions AnsweredDocument9 pagesCushing'S Syndrome and Cushing'S Disease: Your Questions Answeredmawarni siahaanNo ratings yet
- Reproductive SystemDocument49 pagesReproductive SystemAyro Business CenterNo ratings yet
- Body Types MCQDocument9 pagesBody Types MCQDoha DharewaNo ratings yet
- Nutritional BiochemistryDocument17 pagesNutritional BiochemistryVytheeshwaran Vedagiri100% (13)
- Mother and Daughters GuideDocument6 pagesMother and Daughters GuideJane AndersonNo ratings yet
- Energy Circles 1Document34 pagesEnergy Circles 1Satish Agrawal86% (7)
- 4.3 THE MENSTRUAL CYCLE (Form 1 Science)Document25 pages4.3 THE MENSTRUAL CYCLE (Form 1 Science)RATNAJYOUTI A/P KATHIRESAN Moe100% (1)
- Genetic Predisposition in Type 2 Diabetes A PromisingDocument23 pagesGenetic Predisposition in Type 2 Diabetes A PromisingRa,i Al HaddadNo ratings yet
- JaundiceDocument3 pagesJaundiceNyaoNyao MarcellanaNo ratings yet
- Krok 1 - 2006 (General Medicine) - EneutronDocument58 pagesKrok 1 - 2006 (General Medicine) - EneutronHarsh NimavatNo ratings yet
- Biochemistry IDocument10 pagesBiochemistry IKathiravan Murugesan (Kathir An)No ratings yet
- Lecture Notes-Bioreactor Design and Operation-1Document19 pagesLecture Notes-Bioreactor Design and Operation-1LCtey100% (1)
- WORD ROOTDocument11 pagesWORD ROOTta0606hiroNo ratings yet
- NUR11O1 Integrated Human Anatomy and Physiology Department of Biology Institute of Arts and Sciences Far Eastern UniversityDocument4 pagesNUR11O1 Integrated Human Anatomy and Physiology Department of Biology Institute of Arts and Sciences Far Eastern UniversityPrancheska Abigayle Peneyra SantiagoNo ratings yet
- Week 2 Endocrine Anatomy and Physiology Review & Pituitary DisturbancesDocument27 pagesWeek 2 Endocrine Anatomy and Physiology Review & Pituitary DisturbancesZiqri Dimas SandyNo ratings yet
- Role of Micro-Mineral in Infertility in Dairy CattleDocument23 pagesRole of Micro-Mineral in Infertility in Dairy CattlenaturalamirNo ratings yet
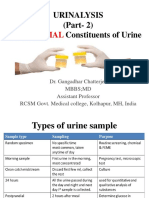
- Urinalysis (Part-2) Constituents of Urine: AbnormalDocument49 pagesUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshNo ratings yet
- Human Digestive SystemDocument19 pagesHuman Digestive SystemCrow LordNo ratings yet
- Mindray Bs 200Document13 pagesMindray Bs 200Roberto AriasNo ratings yet