You might also like
- Man Dragging His ButtDocument2 pagesMan Dragging His ButtJohn Mark PocsidioNo ratings yet
- Financing Quotation NORMAN INNOVA GASDocument1 pageFinancing Quotation NORMAN INNOVA GASJohn Mark PocsidioNo ratings yet
- Financing Quotation NORMAN INNOVA DSLDocument1 pageFinancing Quotation NORMAN INNOVA DSLJohn Mark PocsidioNo ratings yet
- Quote Format - Prulife UK JAN 3 2014Document1 pageQuote Format - Prulife UK JAN 3 2014John Mark PocsidioNo ratings yet
- Quote Format - Prulife UK JAN 3 2014Document1 pageQuote Format - Prulife UK JAN 3 2014John Mark PocsidioNo ratings yet
- Toyota Altis 1.6 G AT OfferDocument1 pageToyota Altis 1.6 G AT OfferJohn Mark PocsidioNo ratings yet
- Quote Format - Prulife UK JAN 3 2014Document1 pageQuote Format - Prulife UK JAN 3 2014John Mark PocsidioNo ratings yet
- Quote Format - Prulife UK JAN 3 2014Document1 pageQuote Format - Prulife UK JAN 3 2014John Mark PocsidioNo ratings yet
- HMDDocument9 pagesHMDJohn Mark PocsidioNo ratings yet
- Quote Format - Prulife UK JAN 3 2014Document1 pageQuote Format - Prulife UK JAN 3 2014John Mark PocsidioNo ratings yet
- Emergency NursingDocument8 pagesEmergency NursingJohn Mark PocsidioNo ratings yet
- Quote Format - Prulife UK JAN 3 2014Document1 pageQuote Format - Prulife UK JAN 3 2014John Mark PocsidioNo ratings yet
- GilbertDocument10 pagesGilbertJohn Mark PocsidioNo ratings yet
- Tetralogy of Fallot ExplainedDocument9 pagesTetralogy of Fallot ExplainedLaurice BarronNo ratings yet
- Newborn CareDocument49 pagesNewborn CareJohn Mark PocsidioNo ratings yet
- Pre-eclampsia Guide: Causes, Symptoms and TreatmentDocument12 pagesPre-eclampsia Guide: Causes, Symptoms and TreatmentJohn Mark PocsidioNo ratings yet
- Tetralogy of Fallot ExplainedDocument9 pagesTetralogy of Fallot ExplainedLaurice BarronNo ratings yet
- Tetralogy of FallotDocument3 pagesTetralogy of FallotJohn Mark PocsidioNo ratings yet
- Pre-eclampsia Guide: Causes, Symptoms and TreatmentDocument12 pagesPre-eclampsia Guide: Causes, Symptoms and TreatmentJohn Mark PocsidioNo ratings yet
- Integumentary DisordersDocument9 pagesIntegumentary DisordersJohn Mark PocsidioNo ratings yet
- GilbertDocument10 pagesGilbertJohn Mark PocsidioNo ratings yet
- Pre-eclampsia Guide: Causes, Symptoms and TreatmentDocument12 pagesPre-eclampsia Guide: Causes, Symptoms and TreatmentJohn Mark PocsidioNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Craftsman - 1903 - 03 - MarchDocument115 pagesThe Craftsman - 1903 - 03 - Marchmdc2013No ratings yet
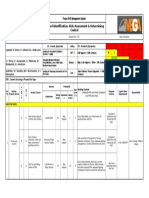
- Risk Assesment SafetyDocument1 pageRisk Assesment SafetyVipin Kumar Parashar100% (1)
- Accident Investigation & Counter MeasuresDocument40 pagesAccident Investigation & Counter MeasuresabdelrahmanNo ratings yet
- Failure Analysis Report v3 - FinalDocument15 pagesFailure Analysis Report v3 - FinalWarren Michael ArthurNo ratings yet
- ExL3 - 100414-2 Lucky Landing in BrazilDocument2 pagesExL3 - 100414-2 Lucky Landing in BrazilantoniomoncadaNo ratings yet
- Hollnagel Is Safety A Subject For ScienceDocument4 pagesHollnagel Is Safety A Subject For ScienceCostaDinos PapadopoulosNo ratings yet
- SPM PHYSICS FORM 4 Forces and MotionDocument16 pagesSPM PHYSICS FORM 4 Forces and MotionJunelle Lau Xia Jiun0% (1)
- ATP CAT Practice QuestionsDocument10 pagesATP CAT Practice QuestionsTayfun TUNAERNo ratings yet
- 2Fast2Furious: The NovelDocument162 pages2Fast2Furious: The NoveldeckfightNo ratings yet
- Describing Road Crash IncidenttDocument10 pagesDescribing Road Crash IncidenttChristopher A JawayNo ratings yet
- Form - LTS New All 2Document1 pageForm - LTS New All 2BluesCreeper OfficialNo ratings yet
- Barge Securing ManualDocument20 pagesBarge Securing ManualTony Francis100% (1)
- Kpi'S Environment, Health and SafetyDocument7 pagesKpi'S Environment, Health and SafetyRobby DamanikNo ratings yet
- Afterlife of Billy Fingers ExcerptDocument12 pagesAfterlife of Billy Fingers ExcerptYady Rosario100% (3)
- Supplementary Notes - Chapter 4 - Lattice VibrationDocument43 pagesSupplementary Notes - Chapter 4 - Lattice VibrationsurendergunalanNo ratings yet
- Birth Time Rectification The Chandra Navamsa Paddathi SystemDocument24 pagesBirth Time Rectification The Chandra Navamsa Paddathi SystemGarga50% (2)
- Contract of IndemnityDocument3 pagesContract of IndemnityPratiksha Jagdish100% (1)
- Industry ReportDocument23 pagesIndustry ReportThameem Abbas100% (1)
- Review of Jude the Obscure and its Controversial ThemesDocument8 pagesReview of Jude the Obscure and its Controversial ThemesŞeyma KayaNo ratings yet
- Knockhardy Kinetics Notes PDFDocument9 pagesKnockhardy Kinetics Notes PDFTigger257No ratings yet
- Try As We Might To Avoid Them, Accidents Happen. Tell Us A Time When You Were Involved in An AccidentDocument4 pagesTry As We Might To Avoid Them, Accidents Happen. Tell Us A Time When You Were Involved in An Accidentapi-129540023No ratings yet
- 20 Effects of Human Behaviors and Geometri Factors in Road Traffic AccidentsDocument10 pages20 Effects of Human Behaviors and Geometri Factors in Road Traffic Accidentsemer_quezonNo ratings yet
- Safety Alert GujaratDocument2 pagesSafety Alert GujaratUnitac HaziiNo ratings yet
- P30 / P30L Pistol: Operator's ManualDocument62 pagesP30 / P30L Pistol: Operator's ManualNikos SakellariouNo ratings yet
- Fill in The Correct Form of The Verb - All Tenses: T TensDocument2 pagesFill in The Correct Form of The Verb - All Tenses: T TensdoushkaNo ratings yet
- Code of Practice For Design and Operationof BoilersDocument85 pagesCode of Practice For Design and Operationof Boilersthawdar100% (1)
- Causal AnalysisDocument9 pagesCausal AnalysisRoger SchulpNo ratings yet
- Hammer Union PresentationDocument17 pagesHammer Union PresentationDaniel100% (1)
- Homeopathic First AidDocument29 pagesHomeopathic First AidHarpreet Saini100% (2)