You might also like
- HPPN 2018 Programme - FinalDocument2 pagesHPPN 2018 Programme - FinalhppnukNo ratings yet
- HPPN 2018 Programme - FinalDocument2 pagesHPPN 2018 Programme - FinalhppnukNo ratings yet
- HPPN 2018 Programme - FinalDocument2 pagesHPPN 2018 Programme - FinalhppnukNo ratings yet
- HPPN 2018 Draft ProgrammeDocument1 pageHPPN 2018 Draft ProgrammehppnukNo ratings yet
- HPPN 2018 Programme - Draft 2Document1 pageHPPN 2018 Programme - Draft 2hppnukNo ratings yet
- HPPN 2018 Draft ProgrammeDocument1 pageHPPN 2018 Draft ProgrammehppnukNo ratings yet
- Imelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandDocument11 pagesImelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandhppnukNo ratings yet
- HPPN 2017 ProgrammeDocument2 pagesHPPN 2017 ProgrammehppnukNo ratings yet
- HPPN 3-4 Sept 12Document2 pagesHPPN 3-4 Sept 12hppnukNo ratings yet
- HPPN Spring Event (24 Apr 2014) - ProgrammeDocument2 pagesHPPN Spring Event (24 Apr 2014) - ProgrammehppnukNo ratings yet
- HPPN Spring Event (24 Apr 2014) - AbstractsDocument7 pagesHPPN Spring Event (24 Apr 2014) - AbstractshppnukNo ratings yet
- HPPN Spring Event (13 Mar 2012) - Conference ProgrammeDocument2 pagesHPPN Spring Event (13 Mar 2012) - Conference ProgrammehppnukNo ratings yet
- HPPN Annual Conference (2-3 Sept 2013)Document2 pagesHPPN Annual Conference (2-3 Sept 2013)hppnukNo ratings yet
- HPPN Abstracts (16 March 2010)Document8 pagesHPPN Abstracts (16 March 2010)hppnukNo ratings yet
- Politics of Health Annual Conference AbstractDocument10 pagesPolitics of Health Annual Conference AbstracthppnukNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- JUALEIA HALLEY and HEATHER GONGAWARE V WaitrDocument22 pagesJUALEIA HALLEY and HEATHER GONGAWARE V WaitrGawker.comNo ratings yet
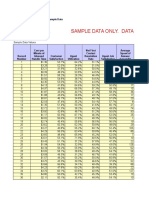
- Sample Call Center Benchmarking Data FileDocument8 pagesSample Call Center Benchmarking Data FilemajiammanathNo ratings yet
- Government AccountingDocument2 pagesGovernment AccountingLloyd SonicaNo ratings yet
- CNO Urged to Change NCLEX Retake, Temporary Registration PoliciesDocument4 pagesCNO Urged to Change NCLEX Retake, Temporary Registration PolicieskennthisraelNo ratings yet
- School:: Last Name First Name Middle Name School AttendedDocument16 pagesSchool:: Last Name First Name Middle Name School AttendedPhilBoardResultsNo ratings yet
- Conflict Management and Negotiation - Team 5Document34 pagesConflict Management and Negotiation - Team 5Austin IsaacNo ratings yet
- SOP Confined Space-ContractorsDocument4 pagesSOP Confined Space-ContractorsAshwinSiddaramaiahNo ratings yet
- Proposed SAIL Pension SchemeDocument2 pagesProposed SAIL Pension Schemeangadpur100% (1)
- Adler (2011) Combining - Collaborative CreativeDocument23 pagesAdler (2011) Combining - Collaborative Creativebherrera1No ratings yet
- 2 - Working Time Regulation 1998Document3 pages2 - Working Time Regulation 1998nnigeltaylorNo ratings yet
- Global Code of Ethics for TourismDocument8 pagesGlobal Code of Ethics for TourismSherrin XieNo ratings yet
- Job Application Letter BanglaDocument4 pagesJob Application Letter Banglajlnggfajd100% (2)
- Model Questions - 2018 - Macroeconomics FinalDocument9 pagesModel Questions - 2018 - Macroeconomics FinalSomidu ChandimalNo ratings yet
- 57.emmanuel D. Quintanar, Et Al., vs. Coca-Cola Bottlers, Philippines, Inc., G.R. No. 210565, 28 June 201Document2 pages57.emmanuel D. Quintanar, Et Al., vs. Coca-Cola Bottlers, Philippines, Inc., G.R. No. 210565, 28 June 201ErwinNo ratings yet
- Management Process and EffectivenessDocument12 pagesManagement Process and EffectivenessDennis Esik MaligayaNo ratings yet
- Grade 12 NSC Business Studies P1 (English) 2021 Preparatory Examination Question PaperDocument10 pagesGrade 12 NSC Business Studies P1 (English) 2021 Preparatory Examination Question PaperTshwaneloNo ratings yet
- Professor: Dr. Felina C. YoungDocument8 pagesProfessor: Dr. Felina C. YoungS DNo ratings yet
- State of Indian Agriculture, 2015-16Document280 pagesState of Indian Agriculture, 2015-16Ayan PaulNo ratings yet
- Hasang Hydro Power Plant Generates 275 GWh AnnuallyDocument62 pagesHasang Hydro Power Plant Generates 275 GWh AnnuallyMark Jayson Baes NamucoNo ratings yet
- Pal Vs ZamoraDocument10 pagesPal Vs ZamorapyulovincentNo ratings yet
- B 1Document16 pagesB 1farhen saledinNo ratings yet
- Incentives Provided by Indian GovernmentDocument6 pagesIncentives Provided by Indian GovernmentDivyam ShahNo ratings yet
- Labour Law AssignmentDocument13 pagesLabour Law Assignmentshivam madhwaniNo ratings yet
- A Merit-Based Pay System For BC Teachers?: Sandy Hirtz of CEET BC Asked This Question Over at TheDocument3 pagesA Merit-Based Pay System For BC Teachers?: Sandy Hirtz of CEET BC Asked This Question Over at TheFarwah IqbalNo ratings yet
- GB520 Unit 3 Case AnalysisDocument9 pagesGB520 Unit 3 Case AnalysisKatherine Moore GageNo ratings yet
- Reading and Writing ResumeDocument34 pagesReading and Writing ResumeFranxlNo ratings yet
- Lecture 1 IntroductionDocument36 pagesLecture 1 IntroductionLouis WongNo ratings yet
- HRM Honda Case Group 6Document10 pagesHRM Honda Case Group 6venkatdeepakvbNo ratings yet
- Chamber Business Magazine - Sept & Oct 2011Document16 pagesChamber Business Magazine - Sept & Oct 2011Cadillac Area Chamber of CommerceNo ratings yet
- Final Project On Aquasure Packaged Drinking Water.Document53 pagesFinal Project On Aquasure Packaged Drinking Water.Rahul Rathore67% (3)