You might also like
- Morphopathology SET 16 Pathologies of The Gastrointestinal TractDocument29 pagesMorphopathology SET 16 Pathologies of The Gastrointestinal TractMohammad_Islam87No ratings yet
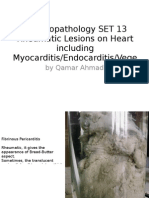
- Morphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeDocument25 pagesMorphopathology SET 13 Rheumatic Lesions On Heart Including Myocarditis/Endocarditis/VegeMohammad_Islam87No ratings yet
- AnaemiaDocument83 pagesAnaemiaMohammad_Islam87100% (2)
- Lecture 20 CarcinogenesisDocument84 pagesLecture 20 CarcinogenesisMohammad_Islam87100% (1)
- Liver Curs 2009Document215 pagesLiver Curs 2009Mohammad_Islam87No ratings yet
- Morphopathology SET 15 Renal Pathologies: by Qamar AhmadDocument25 pagesMorphopathology SET 15 Renal Pathologies: by Qamar AhmadMohammad_Islam87No ratings yet
- Morphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadDocument19 pagesMorphopathology SET 12 Cardiomyopathy (Ischemic) : by Qamar AhmadMohammad_Islam87No ratings yet
- Morphopathology Macroscopy (Romanian-Batch)Document187 pagesMorphopathology Macroscopy (Romanian-Batch)Mohammad_Islam87100% (1)
- Morphopathology SET14 Respiratory Pathologies: by Qamar AhmadDocument18 pagesMorphopathology SET14 Respiratory Pathologies: by Qamar AhmadMohammad_Islam87No ratings yet
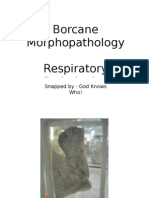
- Borcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument11 pagesBorcane Morphopathology Respiratory Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87No ratings yet
- ?#ry%oefr: - J4 @,8/ MryDocument15 pages?#ry%oefr: - J4 @,8/ MryMohammad_Islam87No ratings yet
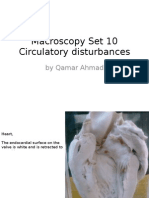
- Macroscopy Set 10 Circulatory Disturbances: by Qamar AhmadDocument55 pagesMacroscopy Set 10 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87No ratings yet
- Borcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument7 pagesBorcane Morphopathology Liver Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87100% (1)
- Workshop 19Document3 pagesWorkshop 19Mohammad_Islam87No ratings yet
- Conditions Presenting With Abdominal PainDocument69 pagesConditions Presenting With Abdominal PainaimanNo ratings yet
- Borcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarDocument7 pagesBorcane Morphopathology Various Pathologies: Snapped By: God Knows Who! Compiled By: QamarMohammad_Islam87No ratings yet
- Workshop 20Document2 pagesWorkshop 20Mohammad_Islam87No ratings yet
- Morphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadDocument24 pagesMorphopatholgy Set 9 Circulatory Disturbances: by Qamar AhmadMohammad_Islam87No ratings yet
- Physical Signs of The AbdomenDocument93 pagesPhysical Signs of The AbdomenaimanNo ratings yet
- Workshop 18Document4 pagesWorkshop 18Mohammad_Islam87No ratings yet
- Morphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersDocument21 pagesMorphopathology Set 11 Atherosclerosis and Other Cardiaovascular DisordersMohammad_Islam87No ratings yet
- Morphopathology Set 8 Melanocytic Tumors: by Qamar AhmadDocument54 pagesMorphopathology Set 8 Melanocytic Tumors: by Qamar AhmadMohammad_Islam87No ratings yet
- STOMACCURS2Document12 pagesSTOMACCURS2Mohammad_Islam87No ratings yet
- Workshop 17Document4 pagesWorkshop 17Mohammad_Islam87No ratings yet
- Stomach - GastritisDocument22 pagesStomach - GastritisaimanNo ratings yet
- Examination of AbdomenDocument41 pagesExamination of AbdomenMohammad_Islam87No ratings yet
- Peptic Ulcer DiseaseDocument54 pagesPeptic Ulcer DiseaseMohammad_Islam87No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Mercury Toxicity and Systemic Elimination Agents Mercola KlinghartDocument10 pagesMercury Toxicity and Systemic Elimination Agents Mercola KlinghartzaskribdoNo ratings yet
- ErythromycinDocument1 pageErythromycinKenneth Robert Abrantes0% (1)
- BSC Nursing: Medical Surgical Nursing - I Unit V - Disorders of The Cardio Vascular SystemDocument36 pagesBSC Nursing: Medical Surgical Nursing - I Unit V - Disorders of The Cardio Vascular SystemPoova RagavanNo ratings yet
- NLE: Community Health Nursing Exam 1: Text ModeDocument33 pagesNLE: Community Health Nursing Exam 1: Text ModeAngelica SorianoNo ratings yet
- Acoustic NeuromaDocument14 pagesAcoustic NeuromaNeshanth SurendranNo ratings yet
- Active and Passive Euthanasia Thesis StatementDocument7 pagesActive and Passive Euthanasia Thesis StatementDoMyPaperForMeSingapore100% (2)
- Sop For Public HealthDocument1 pageSop For Public HealthAyomiposi OloniniyiNo ratings yet
- 29 RAMOS V CA (v2)Document2 pages29 RAMOS V CA (v2)sarah_trinidad_11No ratings yet
- SPC 124433Document5 pagesSPC 124433abdelaziz_ismail685662No ratings yet
- Alcohol and PancreatitisDocument2 pagesAlcohol and Pancreatitishrpwmv83No ratings yet
- PhysioEx9,1: Exercise 7 Activity 2: PEX-07-02Document8 pagesPhysioEx9,1: Exercise 7 Activity 2: PEX-07-02mishael_baig100% (11)
- Diabetic NeuropathyDocument31 pagesDiabetic NeuropathyDEWI RIZKI AGUSTINANo ratings yet
- Velez College Cebu City, Philippines: GEC - PC GEC - MMW Pmls 1Document3 pagesVelez College Cebu City, Philippines: GEC - PC GEC - MMW Pmls 1Armyl Raul CanadaNo ratings yet
- Different Therepeutic Category of Drugs and Its Example Drug ProductsDocument8 pagesDifferent Therepeutic Category of Drugs and Its Example Drug ProductsGermie PosionNo ratings yet
- Assessment of The Lower LimbDocument496 pagesAssessment of The Lower Limbkacheren100% (4)
- Pronation TherapyDocument26 pagesPronation TherapyydtrgnNo ratings yet
- Cesarean Delivery: Postoperative Issues - UpToDateDocument12 pagesCesarean Delivery: Postoperative Issues - UpToDateZurya UdayanaNo ratings yet
- Issues in Psychotherapy With Terminally Ill PatientsDocument9 pagesIssues in Psychotherapy With Terminally Ill PatientsanaghaNo ratings yet
- First AidDocument33 pagesFirst AidRoseMarie MasongsongNo ratings yet
- Sepsis EncephalopathyDocument10 pagesSepsis EncephalopathyMarco Antonio KoffNo ratings yet
- Pulse Diagnosis of Chinese MedicineDocument69 pagesPulse Diagnosis of Chinese MedicineYanikdj100% (3)
- Postoperative Care in MedicalDocument5 pagesPostoperative Care in MedicalMark Russel Sean LealNo ratings yet
- Peds Exam 2 Review QuestionsDocument11 pagesPeds Exam 2 Review Questionschristalh7460% (5)
- Neuro-Onkologi: Bagian/SMF Saraf FK-UGM/RS Dr. Sardjito YogyakartaDocument59 pagesNeuro-Onkologi: Bagian/SMF Saraf FK-UGM/RS Dr. Sardjito YogyakartaNovasiska Indriyani HutajuluNo ratings yet
- Mental Health ActDocument20 pagesMental Health ActBiswas AruNo ratings yet
- Case in Herniorraphy BESTCASEDocument23 pagesCase in Herniorraphy BESTCASEAdrian MallarNo ratings yet
- New Patient Registration PacketDocument11 pagesNew Patient Registration PacketDan DrambareanuNo ratings yet
- 2 תרגול YY Gyneco-OncologyDocument191 pages2 תרגול YY Gyneco-OncologyTarek TarekNo ratings yet
- Extraoral Radiography PDFDocument2 pagesExtraoral Radiography PDFJackNo ratings yet
- Q1 Las Health10 Module1 WK1 - 2Document10 pagesQ1 Las Health10 Module1 WK1 - 2bonzai guillenaNo ratings yet