Practical issues in therapeutic hypothermia
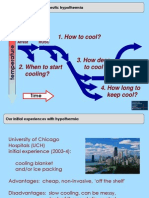
Practical issues of cooling
1. How to cool?
Arrest ROSC
temperature
2. When to start cooling?
3. How deep to cool?
Time time
4. How long to keep cool?
Our initial experiences with hypothermia
How to cool?
University of Chicago Hospitals (UCH) initial experience (2003-4): cooling blanket and/or ice packing Advantages: cheap, non-invasive, off the shelf Disadvantages: slow cooling, can be messy, lack of thermostatic control
Overcooling using ice for hypothermia
Difficulties with ice bag cooling
Merchant RM et al, 2006 Retrospective chart review of cooling cases From three hospitals (2 in U.S., 1 in U.K.) Found 20/32 cases (63%) were overcooled
Trends towards better outcome in non-overcooled pts
Suggests need for thermostatic feedback control
An example of a patient cooled with ice
Surface cooling in the real world
40 39 38
Example A
Temperature (Celsius)
37 36 35 34 33 32 31 30 29 0 4 8 12 16 Time (hours) 20 24 28 32
Merchant RM et al, 2006
What about cold intravenous fluids?
Is cold saline enough?
Cold infusions alone are effective for induction of therapeutic Hypothermia but do not keep patients cool after cardiac arrest
But maintenance was hard Kliegel et al, 2007
Cooling was fast
65% cooled to target within 60 minutes 77% failed to stay cool during course
An example from the real world of cooling patients
Real world usage: Switzerland
From evidence to clinical practice: Effective implementation of therapeutic hypothermia to improve patient outcome after cardiac arrest Oddo et al, Critical Care Medicine 2006 Oddo M et al, 2006
Study at one hospital in Switzerland
Survivors of out-of-hospital arrest
Cooling initially via ice bags, then cooling mattress Target temperature 33oC, maintained for 24 hrs
A real world example: cerebral performance category (CPC) outcomes
Real world usage: Switzerland
Outcome at discharge for out-of-hospital VF arrest
baseline cooling
CPC5 56% CPC 5 40%
.CPC3
CPC3 19% CPC2 14%
CPC2 12% CPC1 42%
CPC1 14%
5%
A real world example: cerebral performance category (CPC) outcomes Real world usage: Switzerland
Outcome at discharge for out-of-hospital asystole arrest
baseline
CPC5 89%
CPC3 11%
cooling
CPC5 83%
CPC1 17%
Post-arrest care is more than just cooling
Post-arrest care is a critical care bundle: Therapeutic hypothermia
Careful blood pressure management
Treatment for coronary blockages Brain and outcomes assessment
A public resource for more hypothermia information
Hypothermia resource website
www.med.upenn.edu/resuscitation/Hypothermia.htm
Training program for health care providers
Hypothermia Training Institute at Penn Philadelphia next course March, 2013 Intensive two day CME course in hypothermia methods, protocols, and applications Designed for critical care, cardiology or emergency medicine physicians and nurse managers i.e., local champions Offers hypothermia certification Workshop design small course size held quarterly
Upcoming Coursera lectures in this program
Lecture 2: Lecture 3:
Rethinking CPR: quality of care and new ideas about training Therapeutic hypothermia and postresuscitation care Frontiers in resuscitation: reperfusion medicine and cardiac bypass Survivorship and end-of-life issues after cardiac arrest
Lecture 4: Lecture 5:
You might also like
- The Rising Popularity of Dystopian LiteratureDocument2 pagesThe Rising Popularity of Dystopian LiteratureaiuzuNo ratings yet
- Virulence FactorsDocument5 pagesVirulence FactorsaiuzuNo ratings yet
- Blood Stain Pattern AnalysisDocument14 pagesBlood Stain Pattern Analysisaiuzu100% (1)
- InformedConsent QualitativestudiesDocument9 pagesInformedConsent QualitativestudiesaiuzuNo ratings yet
- AB Prema Jacini DejstvaDocument2 pagesAB Prema Jacini DejstvaAna SaricNo ratings yet
- Link Click-English TestDocument10 pagesLink Click-English TestKristinaAndrićNo ratings yet
- IXSSrjesenjaDocument3 pagesIXSSrjesenjaaiuzuNo ratings yet
- German WordsDocument8 pagesGerman WordsaiuzuNo ratings yet
- Uho - Organ Sluha I RavnoteDocument6 pagesUho - Organ Sluha I RavnoteaiuzuNo ratings yet
- IXSSrjesenjaDocument3 pagesIXSSrjesenjaaiuzuNo ratings yet
- ISS2014 ApplicationForm STDocument5 pagesISS2014 ApplicationForm STaiuzuNo ratings yet
- Instructions For Europass CVDocument12 pagesInstructions For Europass CVKasia KowalskaNo ratings yet
- Instructions For Europass CVDocument12 pagesInstructions For Europass CVKasia KowalskaNo ratings yet
- Link Click-English TestDocument10 pagesLink Click-English TestKristinaAndrićNo ratings yet
- PrepositionsDocument3 pagesPrepositionsaiuzuNo ratings yet
- English IdiomsDocument1 pageEnglish IdiomsaiuzuNo ratings yet
- Slides ROSC Lecture 3 Part 3Document12 pagesSlides ROSC Lecture 3 Part 3aiuzuNo ratings yet
- Slides ROSC Lecture 2 Part 3Document13 pagesSlides ROSC Lecture 2 Part 3aiuzuNo ratings yet
- Cooling The Body To Save The Heart and Brain: Therapeutic Hypothermia After Cardiac ArrestDocument21 pagesCooling The Body To Save The Heart and Brain: Therapeutic Hypothermia After Cardiac ArrestaiuzuNo ratings yet
- English IdiomsDocument1 pageEnglish IdiomsaiuzuNo ratings yet
- Slides ROSC Lecture 3 Part 3Document12 pagesSlides ROSC Lecture 3 Part 3aiuzuNo ratings yet
- The Action Potential: Page 1. IntroductionDocument12 pagesThe Action Potential: Page 1. IntroductionSimón JimenezNo ratings yet
- Membrane PotentialDocument10 pagesMembrane PotentialaiuzuNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)