You might also like
- 04-Sikaroodi Et AlDocument4 pages04-Sikaroodi Et AlGustavoNo ratings yet
- Familial Takayasu Arteritis - A Pediatric Case and A Review of The LiteratureDocument5 pagesFamilial Takayasu Arteritis - A Pediatric Case and A Review of The LiteratureGustavoNo ratings yet
- 1757 1626 1 52Document5 pages1757 1626 1 52GustavoNo ratings yet
- 1883 10878 1 PBDocument6 pages1883 10878 1 PBGustavoNo ratings yet
- Water Its Importance To LifeDocument6 pagesWater Its Importance To LifeGustavoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Coronary Angiogram Leaflet (Compatibility MoDocument2 pagesCoronary Angiogram Leaflet (Compatibility MoAgnesthesiaNo ratings yet
- TestBank c1Document7 pagesTestBank c1rehab ebraheemNo ratings yet
- Gold Standards in Medical FieldDocument8 pagesGold Standards in Medical FieldJyothisankar Radhakrishnan100% (2)
- Chronic Total Occlusions: Emmanouil S. Brilakis, MD, PHDDocument69 pagesChronic Total Occlusions: Emmanouil S. Brilakis, MD, PHDсергейNo ratings yet
- Ajr 07 2491Document6 pagesAjr 07 2491Khalvia KhairinNo ratings yet
- Bo Gao, Hongjun Li, Meng Law - Imaging of CNS Infections and Neuroimmunology (2019, Springer Singapore)Document215 pagesBo Gao, Hongjun Li, Meng Law - Imaging of CNS Infections and Neuroimmunology (2019, Springer Singapore)Rini WidyantariNo ratings yet
- Vascular InjuryDocument85 pagesVascular InjuryWildaNo ratings yet
- Imaging and RadiologyDocument7 pagesImaging and RadiologyOdyNo ratings yet
- Madsen 2013Document7 pagesMadsen 2013Rafael Mujica OreNo ratings yet
- What Is An Arteriovenous Malformation (AVM) ?Document4 pagesWhat Is An Arteriovenous Malformation (AVM) ?Rafika MonalisaNo ratings yet
- Dust inDocument7 pagesDust inlarkspor31No ratings yet
- Optopol Revo OCT User Manual 11.5.1Document387 pagesOptopol Revo OCT User Manual 11.5.1Chee Yuan LokNo ratings yet
- ZRVS - MedicineDocument19 pagesZRVS - MedicineAbdul0% (1)
- Imaging For Students - Lisle, David A.Document307 pagesImaging For Students - Lisle, David A.Elenanana100% (17)
- Brochure Optima IGS 330 2016Document7 pagesBrochure Optima IGS 330 2016Mauricio Ernesto Andrade MaquilónNo ratings yet
- Ijcset V1Document412 pagesIjcset V1excelingtechNo ratings yet
- Dick Quinn - Left For Dead - Cayenne Pepper-R F Quinn Pub Co (1991)Document212 pagesDick Quinn - Left For Dead - Cayenne Pepper-R F Quinn Pub Co (1991)Gleb Pogaday100% (1)
- Pachychoroid PDFDocument9 pagesPachychoroid PDFRima HajjarNo ratings yet
- Sheath Guidewire Dan CathetersDocument40 pagesSheath Guidewire Dan CathetersMabro CahyoNo ratings yet
- Natural Therapy For Opening The Veins of The HeartDocument2 pagesNatural Therapy For Opening The Veins of The Heartsachinjadhav777No ratings yet
- ACIST Contrast Delivery System Service Manual: and CMS2000 and VoyagerDocument114 pagesACIST Contrast Delivery System Service Manual: and CMS2000 and VoyagerSvilen PopovNo ratings yet
- OrthoDocument148 pagesOrthoCess KimNo ratings yet
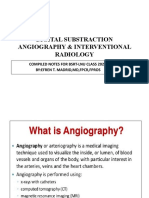
- DIGITAL SUBSTRACTION ANGIOGRAPHY & INTERVENTIONAL RADIOLOGYnewDocument79 pagesDIGITAL SUBSTRACTION ANGIOGRAPHY & INTERVENTIONAL RADIOLOGYnewDaniel MontesNo ratings yet
- Angiografi Femoralis-1Document24 pagesAngiografi Femoralis-1Sepahit Kopi Hitam100% (1)
- The Automatic Fluorescein Angiography SystemDocument3 pagesThe Automatic Fluorescein Angiography SystemHamza ElmbarkiNo ratings yet
- Medical Imaging Units SpecsDocument12 pagesMedical Imaging Units Specsar nedungadiNo ratings yet
- Interventional Radiology: The Principles of Subtraction Are Based On The FollowingDocument4 pagesInterventional Radiology: The Principles of Subtraction Are Based On The FollowingAinne Joy DimapilisNo ratings yet
- ArrowDocument12 pagesArrowcelestialionNo ratings yet
- Radiology MCQSDocument23 pagesRadiology MCQSHabib Mughal67% (3)
- CircleCVI-The 10-Min CMR Scan Business Opportunity AssessmentDocument58 pagesCircleCVI-The 10-Min CMR Scan Business Opportunity AssessmentQiao WeiNo ratings yet