You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Nuevo Documento de TextoDocument1 pageNuevo Documento de TextoanotherleecherNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Lun 4 de Mar - Vie 8 de Mar de 2013 (Santiago) Clases Inacap (Sección 37)Document1 pageLun 4 de Mar - Vie 8 de Mar de 2013 (Santiago) Clases Inacap (Sección 37)anotherleecherNo ratings yet
- Anatomy of A Lab ReportDocument3 pagesAnatomy of A Lab ReportanotherleecherNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Colonic Fermentation. A Neglected Topic in Human Physiology EducationDocument2 pagesColonic Fermentation. A Neglected Topic in Human Physiology EducationanotherleecherNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Cambridge Declaration On ConsciousnessDocument2 pagesThe Cambridge Declaration On ConsciousnessPatrik NazarioNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- A System For Fast, Full-Text Entry For Small Electronic DevicesDocument8 pagesA System For Fast, Full-Text Entry For Small Electronic DevicesanotherleecherNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Spotlight Effect in Social Judgment. An Egocentric Bias in Estimates of The Salience of One's Own Actions and AppearanceDocument12 pagesThe Spotlight Effect in Social Judgment. An Egocentric Bias in Estimates of The Salience of One's Own Actions and AppearanceanotherleecherNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Wood (Dead and Alive. Beliefs in Contradictory Conspiracy Theories) (2012)Document8 pagesWood (Dead and Alive. Beliefs in Contradictory Conspiracy Theories) (2012)anotherleecherNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Religious Belief Systems of Persons With High Functioning AutismDocument5 pagesReligious Belief Systems of Persons With High Functioning AutismanotherleecherNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Bacterium That Can Grow by Using Arsenic Instead of PhosphorusDocument16 pagesA Bacterium That Can Grow by Using Arsenic Instead of PhosphorusanotherleecherNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- SEBI Circular Dated 22.08.2011 (Cirmirsd162011)Document3 pagesSEBI Circular Dated 22.08.2011 (Cirmirsd162011)anantNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Theories of Economic Growth ReportDocument5 pagesTheories of Economic Growth ReportAubry BautistaNo ratings yet
- Moparm Action - December 2014 USADocument100 pagesMoparm Action - December 2014 USAenricoioNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Criminal Law I Green Notes PDFDocument105 pagesCriminal Law I Green Notes PDFNewCovenantChurchNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Ahakuelo IndictmentDocument24 pagesAhakuelo IndictmentHNNNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- CE5215-Theory and Applications of Cement CompositesDocument10 pagesCE5215-Theory and Applications of Cement CompositesSivaramakrishnaNalluriNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
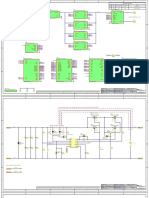
- Scheme Bidirectional DC-DC ConverterDocument16 pagesScheme Bidirectional DC-DC ConverterNguyễn Quang KhoaNo ratings yet
- Annisha Jain (Reporting Manager - Rudrakshi Kumar)Document1 pageAnnisha Jain (Reporting Manager - Rudrakshi Kumar)Ruchi AgarwallNo ratings yet
- DTMF Controlled Robot Without Microcontroller (Aranju Peter)Document10 pagesDTMF Controlled Robot Without Microcontroller (Aranju Peter)adebayo gabrielNo ratings yet
- LISTA Nascar 2014Document42 pagesLISTA Nascar 2014osmarxsNo ratings yet
- Fire and Life Safety Assessment ReportDocument5 pagesFire and Life Safety Assessment ReportJune CostalesNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gowtham Kumar Chitturi - HRMS Technical - 6 YrsDocument4 pagesGowtham Kumar Chitturi - HRMS Technical - 6 YrsAnuNo ratings yet
- Crivit IAN 89192 FlashlightDocument2 pagesCrivit IAN 89192 FlashlightmNo ratings yet
- Flyer Manuale - CON WATERMARK PAGINE SINGOLEDocument6 pagesFlyer Manuale - CON WATERMARK PAGINE SINGOLEjscmtNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- OOPS Notes For 3rd Sem ALL ChaptersDocument62 pagesOOPS Notes For 3rd Sem ALL Chaptersabhishek singh83% (6)
- A.2 de - La - Victoria - v. - Commission - On - Elections20210424-12-18iwrdDocument6 pagesA.2 de - La - Victoria - v. - Commission - On - Elections20210424-12-18iwrdCharisse SarateNo ratings yet
- Pradhan Mantri Gramin Digital Saksharta Abhiyan (PMGDISHA) Digital Literacy Programme For Rural CitizensDocument2 pagesPradhan Mantri Gramin Digital Saksharta Abhiyan (PMGDISHA) Digital Literacy Programme For Rural Citizenssairam namakkalNo ratings yet
- Coursework For ResumeDocument7 pagesCoursework For Resumeafjwdxrctmsmwf100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- SOP No. 6Document22 pagesSOP No. 6Eli CohenNo ratings yet
- Developments in Prepress Technology (PDFDrive)Document62 pagesDevelopments in Prepress Technology (PDFDrive)Sur VelanNo ratings yet
- Nasoya FoodsDocument2 pagesNasoya Foodsanamta100% (1)
- Unit List MUZAFFARPUR - Feb 18 PDFDocument28 pagesUnit List MUZAFFARPUR - Feb 18 PDFPawan Kumar100% (1)
- Computer System Sevicing NC Ii: SectorDocument44 pagesComputer System Sevicing NC Ii: SectorJess QuizzaganNo ratings yet
- Teralight ProfileDocument12 pagesTeralight ProfileMohammed TariqNo ratings yet
- CENT - Company Presentation Q1 2020 PDFDocument22 pagesCENT - Company Presentation Q1 2020 PDFsabrina rahmawatiNo ratings yet
- La Bugal-b'Laan Tribal Association Et - Al Vs Ramos Et - AlDocument6 pagesLa Bugal-b'Laan Tribal Association Et - Al Vs Ramos Et - AlMarlouis U. PlanasNo ratings yet
- How Can You Achieve Safety and Profitability ?Document32 pagesHow Can You Achieve Safety and Profitability ?Mohamed OmarNo ratings yet
- I.V. FluidDocument4 pagesI.V. FluidOdunlamiNo ratings yet
- 16 Easy Steps To Start PCB Circuit DesignDocument10 pages16 Easy Steps To Start PCB Circuit DesignjackNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Double Inlet Airfoil Fans - AtzafDocument52 pagesDouble Inlet Airfoil Fans - AtzafDaniel AlonsoNo ratings yet