You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CancerDocument228 pagesCancerCrystal Grace100% (1)
- Pigment Cell Melanoma Res - 2021 - Talty - The Role of Ferroptosis in Melanoma PDFDocument9 pagesPigment Cell Melanoma Res - 2021 - Talty - The Role of Ferroptosis in Melanoma PDFAnouarNo ratings yet
- Breast Cancer: Presented By: Ola NemriDocument46 pagesBreast Cancer: Presented By: Ola NemriHaitham Ahmed100% (1)
- Lung CancerDocument5 pagesLung CancerAlliah RodriguezNo ratings yet
- Chapter4 Modifiable Risk Factors of Lifestyle DiseasesDocument15 pagesChapter4 Modifiable Risk Factors of Lifestyle DiseasesJohn Kennith Cacho Benlot100% (2)
- Adenomyoepithelioma of The Breast: A Brief Diagnostic ReviewDocument5 pagesAdenomyoepithelioma of The Breast: A Brief Diagnostic ReviewSFCHIKINo ratings yet
- Cancer Management in Man Cancer Management in Man Cancer Management in ManDocument305 pagesCancer Management in Man Cancer Management in Man Cancer Management in Manmanu98kkskskskskiwyhNo ratings yet
- Review On Canine Oral Melanoma: An Undervalued Authentic Genetic Model of Human Oral Melanoma?Document9 pagesReview On Canine Oral Melanoma: An Undervalued Authentic Genetic Model of Human Oral Melanoma?Equilibrium EduardoNo ratings yet
- Paper Canabis Potencial Terapeutico InglesDocument9 pagesPaper Canabis Potencial Terapeutico InglesFRANCISCA ALICIA JADUE ARÉVALONo ratings yet
- Oropharyngeal Cancer: Current Understanding and ManagementDocument7 pagesOropharyngeal Cancer: Current Understanding and ManagementbgdNo ratings yet
- ESP Lisabona 2013 AbstractsDocument252 pagesESP Lisabona 2013 AbstractsstripandslipNo ratings yet
- AJCC Cancer Staging Form Supplement PDFDocument520 pagesAJCC Cancer Staging Form Supplement PDFopi akbarNo ratings yet
- CVDocument46 pagesCVRosnah Binti ZainNo ratings yet
- Prognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPDocument11 pagesPrognostic Indicators in Differentiated Thyroid Carcinoma: Diana S. Dean, MD, and Ian D. Hay, MB, PHD, FRCPRum Afida RasfaNo ratings yet
- Brain Tumor: Basics .. What Is Primary Brain Tumor ?. Initiating Care Plan For Primary Brain Tumor PatientDocument20 pagesBrain Tumor: Basics .. What Is Primary Brain Tumor ?. Initiating Care Plan For Primary Brain Tumor Patientahmed_alkiadyNo ratings yet
- Neoplasm 20&20 Metabolic 20 DiseasesDocument30 pagesNeoplasm 20&20 Metabolic 20 DiseasesSaraNo ratings yet
- AssessmentDocument5 pagesAssessmentshujin_sama100% (2)
- RiordanIVCprotocol enDocument17 pagesRiordanIVCprotocol enPerparim RexhallariNo ratings yet
- ThyroidDocument102 pagesThyroidfadoNo ratings yet
- Ef Ficacy and Safety of Stereotactic Body Radiation Therapy For Pediatric Malignancies: The LITE-SABR Systematic Review and Meta-AnalysisDocument12 pagesEf Ficacy and Safety of Stereotactic Body Radiation Therapy For Pediatric Malignancies: The LITE-SABR Systematic Review and Meta-AnalysisRaul Matute MartinNo ratings yet
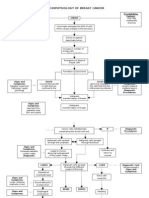
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Basic Principles in Surgical Oncology - Cady1997 Arch Surg PDFDocument9 pagesBasic Principles in Surgical Oncology - Cady1997 Arch Surg PDFDiego EskinaziNo ratings yet
- Cancerul Si NeoplaziaDocument28 pagesCancerul Si NeoplaziaBogdan SoltuzuNo ratings yet
- Case Report: Urachal Adenocarcinoma: A Case Report With Key Imaging Findings and Radiologic-Pathologic CorrelationDocument6 pagesCase Report: Urachal Adenocarcinoma: A Case Report With Key Imaging Findings and Radiologic-Pathologic Correlationchristian hansNo ratings yet
- Composite Hemangioendothelioma An Unusual Presentation of A Rare Vascular TumorDocument5 pagesComposite Hemangioendothelioma An Unusual Presentation of A Rare Vascular TumorTian Nopita SariNo ratings yet
- Poster PPT OssnDocument12 pagesPoster PPT OssnShilpa B KNo ratings yet
- (Springer) Cancer Immunology A Translational Medicine ContextDocument633 pages(Springer) Cancer Immunology A Translational Medicine ContextManoj PandreNo ratings yet
- How Cancer Spreads MetastasisDocument6 pagesHow Cancer Spreads MetastasisAfia TawiahNo ratings yet
- Oncology BulletsDocument11 pagesOncology BulletsDonaJeanNo ratings yet
- (Encyclopedia of Pathology) Pieter J. Slootweg (Eds.) - Dental and Oral Pathology-Springer International Publishing (2016)Document372 pages(Encyclopedia of Pathology) Pieter J. Slootweg (Eds.) - Dental and Oral Pathology-Springer International Publishing (2016)Maria Mery Garcia VelascoNo ratings yet