You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Brain Edema XVI - Translate Basic Science Into Clinical Practice by Richard L Applegate, Gang Chen, Hua Feng, John H. ZhangDocument376 pagesBrain Edema XVI - Translate Basic Science Into Clinical Practice by Richard L Applegate, Gang Chen, Hua Feng, John H. ZhangAjie WitamaNo ratings yet
- Leprosy Reactions: The Effect of Gender and Household ContactsDocument5 pagesLeprosy Reactions: The Effect of Gender and Household ContactsAjie WitamaNo ratings yet
- 5-Minute Urology ConsultDocument216 pages5-Minute Urology ConsultAjie WitamaNo ratings yet
- 5-Minute Urology Consult PDFDocument1,082 pages5-Minute Urology Consult PDFAjie Witama0% (1)
- Treatment Duration of Reversal Reaction: A Reappraisal. Back To The PastDocument9 pagesTreatment Duration of Reversal Reaction: A Reappraisal. Back To The PastAjie WitamaNo ratings yet
- Detect Abnormal Labour Early to Prevent Prolonged, Obstructed Labour IssuesDocument14 pagesDetect Abnormal Labour Early to Prevent Prolonged, Obstructed Labour IssueszingioNo ratings yet
- GINA Pocket 2014 Jun11Document32 pagesGINA Pocket 2014 Jun11Gilbert Petrus Richard SamsNo ratings yet
- Micro Anatomical Variations in The Cerebellopontine AngleDocument14 pagesMicro Anatomical Variations in The Cerebellopontine AngleVictor PimentelNo ratings yet
- Chi Kung in Wing Chun Kung Fu - Scott BakerDocument108 pagesChi Kung in Wing Chun Kung Fu - Scott BakerreapermanpangNo ratings yet
- Vol89 Suppl.4 147 6147Document5 pagesVol89 Suppl.4 147 6147Ajie WitamaNo ratings yet
- Hofmeyer ObstCareInLowResourceSettings 2009Document25 pagesHofmeyer ObstCareInLowResourceSettings 2009Ajie WitamaNo ratings yet
- DisabilityMBChild ProportionDocument7 pagesDisabilityMBChild ProportionAjie WitamaNo ratings yet
- Chamberlain's Symptoms and Signs in Clinical Medicine - Gray, David, Houghton, Andrew RDocument504 pagesChamberlain's Symptoms and Signs in Clinical Medicine - Gray, David, Houghton, Andrew RAjie Witama100% (2)
- Maternal Health Interventions and CommoditiesDocument5 pagesMaternal Health Interventions and CommoditiescrushnaNo ratings yet
- 03 Oa Aetiopathogenesis of TypeDocument6 pages03 Oa Aetiopathogenesis of TypeAjie WitamaNo ratings yet
- Primary Neural Leprosy: Systematic Review: Hanseníase Neural Primária: Revisão SistemáticaDocument8 pagesPrimary Neural Leprosy: Systematic Review: Hanseníase Neural Primária: Revisão SistemáticaAjie WitamaNo ratings yet
- Atlas of Leprosy: A NewDocument25 pagesAtlas of Leprosy: A Newgalina sokolovaNo ratings yet
- Teaching Materials and ServicesDocument9 pagesTeaching Materials and ServicesAjie WitamaNo ratings yet
- Clinical StudyDocument8 pagesClinical StudyAjie WitamaNo ratings yet
- MDT FullDocument190 pagesMDT FullAjie WitamaNo ratings yet
- Leprosy and contact surveillance: active screening detects cases earlierDocument6 pagesLeprosy and contact surveillance: active screening detects cases earlierAjie WitamaNo ratings yet
- LR Mar13 1807Document11 pagesLR Mar13 1807Ajie WitamaNo ratings yet
- VANCOUVER Reference Style Guide: NotesDocument6 pagesVANCOUVER Reference Style Guide: NotesMuhammad MoazzamNo ratings yet
- Editorials: Leprosy-A New Look at An Old DiseaseDocument5 pagesEditorials: Leprosy-A New Look at An Old DiseaseAjie WitamaNo ratings yet
- 03 300Document11 pages03 300Ajie WitamaNo ratings yet
- 1516Document3 pages1516Ajie WitamaNo ratings yet
- Lep014 034Document21 pagesLep014 034Ajie WitamaNo ratings yet
- 1.2 Lepers and Leprosy. Dr. J.J. HoffmanDocument4 pages1.2 Lepers and Leprosy. Dr. J.J. HoffmanAjie WitamaNo ratings yet
- Oper Case HoldingDocument3 pagesOper Case HoldingAjie WitamaNo ratings yet
- J Infect Dis.-2012-Sousa-1417-24Document8 pagesJ Infect Dis.-2012-Sousa-1417-24Ajie WitamaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- PHS 371 - Comparative Health Care Systems: Course OverviewDocument8 pagesPHS 371 - Comparative Health Care Systems: Course OverviewJen CarrollNo ratings yet
- Davison, Blankstein, Flett, Neale, Abnormal Psychology, 6th Canadian Edition TestbankDocument65 pagesDavison, Blankstein, Flett, Neale, Abnormal Psychology, 6th Canadian Edition TestbankMahin RahmanNo ratings yet
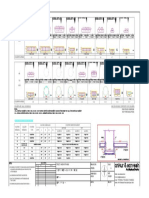
- M30 Reinforced Concrete Column Design DetailsDocument1 pageM30 Reinforced Concrete Column Design DetailsCMM INFRAPROJECTS LTDNo ratings yet
- Best Remedial Center in JaipurDocument15 pagesBest Remedial Center in JaipurLearning Aspiration SchoolNo ratings yet
- Assessment 1 Inclusive EducationDocument10 pagesAssessment 1 Inclusive EducationB NovNo ratings yet
- Disability World 25Document264 pagesDisability World 25Ezekiel T. MostieroNo ratings yet
- NARPAA E-Class Module 3 - Historical Definitions of AutismDocument19 pagesNARPAA E-Class Module 3 - Historical Definitions of AutismnarpaaNo ratings yet
- Supplemental Narrative of Zalonda WoodsDocument7 pagesSupplemental Narrative of Zalonda WoodsJordan Green100% (1)
- Yarra Plenty Regional LibraryDocument49 pagesYarra Plenty Regional LibraryAnonymous zNdbKT993YNo ratings yet
- English Coram Boy EssayDocument3 pagesEnglish Coram Boy EssaySimran SehdevNo ratings yet
- Qantas Disability Access Facilitation PlanDocument60 pagesQantas Disability Access Facilitation PlanFreddieNo ratings yet
- Diap Disability Inclusion Action PlanDocument47 pagesDiap Disability Inclusion Action PlanDorjeNo ratings yet
- Arie Rimmerman-Family Policy and Disability-Cambridge University Press (2015) PDFDocument226 pagesArie Rimmerman-Family Policy and Disability-Cambridge University Press (2015) PDFWederson SantosNo ratings yet
- Registration Form (MIS 03-01) For T2MIS Ver.5 (3!02!18) - 2Document2 pagesRegistration Form (MIS 03-01) For T2MIS Ver.5 (3!02!18) - 2Win P WinNo ratings yet
- Idea Section 504 of The Rehabilitation Act Ada and Essa How A Generation of Learners With Disabilities Were Granted Their RightsDocument5 pagesIdea Section 504 of The Rehabilitation Act Ada and Essa How A Generation of Learners With Disabilities Were Granted Their Rightsapi-529117421No ratings yet
- M Phil Clinical Psychology PDFDocument41 pagesM Phil Clinical Psychology PDFRasmi Ranjan MuduliNo ratings yet
- Designing Randomized, Controlled Trials Aimed at Preventing or Delaying Functional Decline and Disability in Frail, Older Persons: A Consensus ReportDocument10 pagesDesigning Randomized, Controlled Trials Aimed at Preventing or Delaying Functional Decline and Disability in Frail, Older Persons: A Consensus ReportLara Correa BarretoNo ratings yet
- Annual Family Child Care Questionnaire: Instructions: Please Answer The Following Questions Regarding Your Family ChildDocument6 pagesAnnual Family Child Care Questionnaire: Instructions: Please Answer The Following Questions Regarding Your Family Childริดิ พูตราNo ratings yet
- 0005e Group Project Edu 5710Document47 pages0005e Group Project Edu 5710Dayu WiraNo ratings yet
- Dedspled (Idd) 2023Document73 pagesDedspled (Idd) 2023suryafeeds.inNo ratings yet
- NIOS Admission Form - 2013-14Document4 pagesNIOS Admission Form - 2013-14distance_sanjeev100% (1)
- 3Document14 pages3Saurabh PatelNo ratings yet
- Mitigation Declaration For Daniel Wayne CookDocument19 pagesMitigation Declaration For Daniel Wayne CookTucsonSentinelNo ratings yet
- M.K.Jayaraj ReportDocument176 pagesM.K.Jayaraj ReportMas Thulan100% (5)
- Application Form: PersonalDocument6 pagesApplication Form: PersonalasifmengrNo ratings yet
- BME Listening Leirat KözépfokDocument29 pagesBME Listening Leirat KözépfokZoltán Szecsődi100% (1)
- AASW Practice Standards for Social Workers: achieving outcomesDocument32 pagesAASW Practice Standards for Social Workers: achieving outcomesSteven TanNo ratings yet
- Parents Attitude Inclusive Education of Children With DisabilityDocument6 pagesParents Attitude Inclusive Education of Children With Disabilitylazarstosic100% (1)
- DWATCHDocument92 pagesDWATCHFawaz SayedNo ratings yet