You might also like
- Korelasi Antara Geriatric Nutritional Risk Index Dengan Lama Rawat Pasien Geriatri Di Rumah Sakit Sanglah, DenpasarDocument6 pagesKorelasi Antara Geriatric Nutritional Risk Index Dengan Lama Rawat Pasien Geriatri Di Rumah Sakit Sanglah, DenpasarRizki NovitaNo ratings yet
- ARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsDocument5 pagesARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsPPDS Rehab Medik UnhasNo ratings yet
- Mini Nutritional AssessmentDocument7 pagesMini Nutritional AssessmentJoão Mariano SantosNo ratings yet
- Jurnal Reading TerjemahDocument15 pagesJurnal Reading TerjemahLela Nazila ItuSayaNo ratings yet
- Jurnal Amik SanglahDocument6 pagesJurnal Amik Sanglahslamet pujianto SkepNo ratings yet
- Anthropometric Measurement To Identify Undernutrition in Cerabral PalsyDocument8 pagesAnthropometric Measurement To Identify Undernutrition in Cerabral PalsyPam Travezani MiyazakiNo ratings yet
- MNA Original ArticuloDocument22 pagesMNA Original ArticuloHerrera WilberthNo ratings yet
- BIA Rev Med Chil I SCH PDFDocument10 pagesBIA Rev Med Chil I SCH PDFClaudia Avila SáezNo ratings yet
- 2 Year Paleo TrialDocument8 pages2 Year Paleo TrialOfer KulkaNo ratings yet
- Nutritional Assessment Anthropometric MeasurementsDocument4 pagesNutritional Assessment Anthropometric Measurementsশাদ্বলNo ratings yet
- Obesidad en PediatriaDocument17 pagesObesidad en PediatriaAndres Alejandro Cadiz BarreraNo ratings yet
- Comparative Study of Nutritional Status of Elderly Population Living in The Home For Aged Vs Those Living in The CommunityDocument8 pagesComparative Study of Nutritional Status of Elderly Population Living in The Home For Aged Vs Those Living in The CommunityMariya SiddiquiNo ratings yet
- 14 NutritionalDocument57 pages14 NutritionalMulugeta EmiruNo ratings yet
- Larger Thigh and Hip Circumferences Are Associated With Better Glucose ToleranceDocument9 pagesLarger Thigh and Hip Circumferences Are Associated With Better Glucose ToleranceIndah Wati WijayaNo ratings yet
- Relationship Between Mid-Upper Arm Circumference and Body Mass Index in InpatientsDocument10 pagesRelationship Between Mid-Upper Arm Circumference and Body Mass Index in InpatientssyahmiNo ratings yet
- Development and validation of the SNAQr hospital malnutrition screening toolDocument8 pagesDevelopment and validation of the SNAQr hospital malnutrition screening toolDanang Adit KuranaNo ratings yet
- Chapter 2 Nutrition Assessment of AdultsDocument45 pagesChapter 2 Nutrition Assessment of AdultsAmiRa fouziNo ratings yet
- Group 2 Report in NutritionDocument99 pagesGroup 2 Report in Nutritionfe espinosaNo ratings yet
- Chapter Four: - Assessments of CommunityDocument37 pagesChapter Four: - Assessments of CommunityAbdurohaman BelayNo ratings yet
- Media Medika Indonesiana: Tinggi Badan Yang Diukur Dan Berdasarkan Tinggi Lutut Menggunakan Rumus Chumlea Pada LansiaDocument6 pagesMedia Medika Indonesiana: Tinggi Badan Yang Diukur Dan Berdasarkan Tinggi Lutut Menggunakan Rumus Chumlea Pada LansiaPuguh AriefNo ratings yet
- GerantologyDocument6 pagesGerantologyusmanNo ratings yet
- Reliability of Anthropometrie Measurements in OverDocument6 pagesReliability of Anthropometrie Measurements in OverDewi HanaNo ratings yet
- J Rec 2019 07 023 PDFDocument10 pagesJ Rec 2019 07 023 PDFCamilo Armando ROJAS GOMEZNo ratings yet
- Sleep and Dm2Document7 pagesSleep and Dm2Anggi AviandriNo ratings yet
- Altura Promedio en México Estudio de CasoDocument8 pagesAltura Promedio en México Estudio de CasoEddy HarosNo ratings yet
- Post Victoria 2000Document10 pagesPost Victoria 2000julianafurtado1985No ratings yet
- Impact of Nutrition Counselling On Multiple Sclerosis Patients Nutritional Status: Randomized Controlled Clinical TrialDocument19 pagesImpact of Nutrition Counselling On Multiple Sclerosis Patients Nutritional Status: Randomized Controlled Clinical Trialmutiara fajriatiNo ratings yet
- Comparison of Five Malnutrition Screening Tools in One Hospital Inpatient SampleDocument9 pagesComparison of Five Malnutrition Screening Tools in One Hospital Inpatient SampleIka Nadia PrajawatiNo ratings yet
- Dietary counselling and food fortification improves outcomes in COPDDocument7 pagesDietary counselling and food fortification improves outcomes in COPDJames Cojab SacalNo ratings yet
- Nutritional Assessment in Surgical Oncology Patients: A Comparative Analysis Between MethodsDocument6 pagesNutritional Assessment in Surgical Oncology Patients: A Comparative Analysis Between MethodsmelisaberlianNo ratings yet
- 03 - Comparsion of EquationsDocument9 pages03 - Comparsion of EquationsRejanne OliveiraNo ratings yet
- Medidas AntropométricasDocument8 pagesMedidas AntropométricasCarolina JaramilloNo ratings yet
- Abdominal Volume Index. An Anthropometry-Based Index For Estimation of Obesity Is Strongly Related To Impaired Glucose Tolerance and Type 2 Diabetes MellitusDocument5 pagesAbdominal Volume Index. An Anthropometry-Based Index For Estimation of Obesity Is Strongly Related To Impaired Glucose Tolerance and Type 2 Diabetes MellitusNina DorotheaNo ratings yet
- Article AmalDocument16 pagesArticle Amalsaliha mharchiNo ratings yet
- Nutritional AssessmentDocument8 pagesNutritional AssessmentOutour KhNo ratings yet
- BMC Public Health: The Validity of Self-Reported Weight in US Adults: A Population Based Cross-Sectional StudyDocument10 pagesBMC Public Health: The Validity of Self-Reported Weight in US Adults: A Population Based Cross-Sectional Studyteamfrio827No ratings yet
- Waist Circumference and Cardiometabolic Risk: S K, D B. A, S B. H, D E. K, R L. L, C N, R KDocument6 pagesWaist Circumference and Cardiometabolic Risk: S K, D B. A, S B. H, D E. K, R L. L, C N, R KJoni WitziNo ratings yet
- BC Changes in Female Teens with AnorexiaDocument6 pagesBC Changes in Female Teens with AnorexiafitatataNo ratings yet
- Jur DingDocument8 pagesJur DingDeyaSeisoraNo ratings yet
- Nutrition Assessment - 3-1Document59 pagesNutrition Assessment - 3-1tadese kifleNo ratings yet
- Capsulated Proposal-MebmDocument2 pagesCapsulated Proposal-MebmEvette MisagalNo ratings yet
- Obesity and The Risk of Cryptogenic Ischemic Stroke in Young AdultsDocument25 pagesObesity and The Risk of Cryptogenic Ischemic Stroke in Young AdultsKhalilullah ArsyiNo ratings yet
- Adolescent Obesity, Joint Pain, and Hypermobility: Shortreport Open AccessDocument5 pagesAdolescent Obesity, Joint Pain, and Hypermobility: Shortreport Open AccessMCuk2606No ratings yet
- Biochemical and immunological parameters for nutritional screeningDocument9 pagesBiochemical and immunological parameters for nutritional screeningRocio PeñaNo ratings yet
- Rev Bras Hum: CineantropomDocument10 pagesRev Bras Hum: CineantropomJapa Personal TrainerNo ratings yet
- 24 1520325260 - 06-03-2018 PDFDocument9 pages24 1520325260 - 06-03-2018 PDFEditor IJRITCCNo ratings yet
- A Composite Score Combining Waist Circumference and Body Mass Index More Accurately Predicts Body Fat Percentage in 6-To 13-Year-Old ChildrenDocument7 pagesA Composite Score Combining Waist Circumference and Body Mass Index More Accurately Predicts Body Fat Percentage in 6-To 13-Year-Old ChildrenThalia KarampasiNo ratings yet
- Am J Clin Nutr 1975 Gibson 1387 94Document8 pagesAm J Clin Nutr 1975 Gibson 1387 94Chartchai ChaichanaNo ratings yet
- Fnes 368 PresentationDocument13 pagesFnes 368 Presentationapi-702059884No ratings yet
- Frankenfield 2003Document8 pagesFrankenfield 2003Constanza CraNo ratings yet
- Measuring eating behaviorsDocument13 pagesMeasuring eating behaviorsDiogo JuniorNo ratings yet
- Journal - Lung Function Changes in Young Obese Women - A Harbinger For Graver OutcomesDocument6 pagesJournal - Lung Function Changes in Young Obese Women - A Harbinger For Graver OutcomesSondang Farwaty SitanggangNo ratings yet
- A23 AJCN Weight, Shape, and Mortality Risk in Older PersonsDocument12 pagesA23 AJCN Weight, Shape, and Mortality Risk in Older PersonsGabriel CampolinaNo ratings yet
- JAPI Body FatDocument6 pagesJAPI Body FatBhupendra MahantaNo ratings yet
- Migraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesDocument14 pagesMigraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesRetno ManggalihNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryFrom EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryRating: 5 out of 5 stars5/5 (1)
- Ortho 15Document5 pagesOrtho 15azkaparobiNo ratings yet
- Otolaryngology Head and Neck Surgery 2007 Rosenfeld S1 S31Document31 pagesOtolaryngology Head and Neck Surgery 2007 Rosenfeld S1 S31azkaparobiNo ratings yet
- Classification of FracturesDocument9 pagesClassification of FracturesazkaparobiNo ratings yet
- Ophtalmology TerminologyDocument20 pagesOphtalmology TerminologyAlpascaFirdausNo ratings yet
- Magnesium Sulfate Exposure and NeonatalDocument1 pageMagnesium Sulfate Exposure and NeonatalazkaparobiNo ratings yet
- Hyphema MedscapeDocument17 pagesHyphema MedscapeazkaparobiNo ratings yet
- USG HyphemaDocument7 pagesUSG HyphemaazkaparobiNo ratings yet
- Ortho 15Document5 pagesOrtho 15azkaparobiNo ratings yet
- Rheumatic Fever ReviewDocument15 pagesRheumatic Fever ReviewJBNo ratings yet
- Kompetensi ObgynDocument1 pageKompetensi ObgynazkaparobiNo ratings yet
- Nutritional StatusDocument9 pagesNutritional StatusazkaparobiNo ratings yet
- Anthropometric Measurement of The EldelyDocument9 pagesAnthropometric Measurement of The EldelyazkaparobiNo ratings yet
- Basal Cell Carcinoma MedscapeDocument12 pagesBasal Cell Carcinoma MedscapeazkaparobiNo ratings yet
- RAPDDocument2 pagesRAPDAlpascaFirdausNo ratings yet
- Villena 2004Document4 pagesVillena 2004azkaparobiNo ratings yet
- Nutritional Assessment of Elderly Persons in Babylon: Hadeel Fadhil FarhoodDocument8 pagesNutritional Assessment of Elderly Persons in Babylon: Hadeel Fadhil FarhoodazkaparobiNo ratings yet
- Age MalnutritionDocument24 pagesAge MalnutritionazkaparobiNo ratings yet
- Anthropometric Measurement of The EldelyDocument9 pagesAnthropometric Measurement of The EldelyazkaparobiNo ratings yet
- Chronic ConstipationDocument1 pageChronic ConstipationazkaparobiNo ratings yet
- Check List SOCA Blok 10Document6 pagesCheck List SOCA Blok 10Rizka_aprilNo ratings yet
- MCQ Blok 3 2008 RemedialDocument10 pagesMCQ Blok 3 2008 RemedialSuryadi VOoNo ratings yet
- MCQ Blok 4 2007 RemedialDocument15 pagesMCQ Blok 4 2007 RemedialazkaparobiNo ratings yet
- FK FK Blok 6Document15 pagesFK FK Blok 6azkaparobiNo ratings yet
- Quiz Anfis MhsDocument14 pagesQuiz Anfis MhsazkaparobiNo ratings yet
- Born This WayDocument1 pageBorn This WayazkaparobiNo ratings yet
- Leadership Styles of ManagersDocument16 pagesLeadership Styles of ManagersmuzammelNo ratings yet
- In-Circuit and In-Application Programming of The 89C51Rx+/Rx2/66x MicrocontrollersDocument17 pagesIn-Circuit and In-Application Programming of The 89C51Rx+/Rx2/66x Microcontrollersv1swaroopNo ratings yet
- How To Speak English FluentlyDocument7 pagesHow To Speak English Fluentlygermanvip8No ratings yet
- Pre-BASIC VOCABULARY BRILLIANT ENGLISH COURSEDocument7 pagesPre-BASIC VOCABULARY BRILLIANT ENGLISH COURSERisMank Sani QuiCken Heart100% (1)
- Đề thi học kì 2 lớp 8 môn Anh có đáp ánDocument8 pagesĐề thi học kì 2 lớp 8 môn Anh có đáp ánThủy TrầnNo ratings yet
- Aristotle's Works by BEKKER NUMBERS ++++Document2 pagesAristotle's Works by BEKKER NUMBERS ++++parasoly0% (1)
- Guide to Common Japanese Map SymbolsDocument9 pagesGuide to Common Japanese Map SymbolsAfsar HasanNo ratings yet
- 6529XXXXXXXXXX34 01-05-2023 UnlockedDocument2 pages6529XXXXXXXXXX34 01-05-2023 UnlockedSath KNo ratings yet
- Why Jamf?Document3 pagesWhy Jamf?Prakash MaharajNo ratings yet
- Differences in anthropometric characteristics and somatotype in young soccer players and karate practicionersDocument8 pagesDifferences in anthropometric characteristics and somatotype in young soccer players and karate practicionerssyafiqahNo ratings yet
- TS 2030Document289 pagesTS 2030dhmartiniNo ratings yet
- Ewm Class 40 - ScrappingDocument8 pagesEwm Class 40 - ScrappingRaviteja KanakaNo ratings yet
- RRL in ThesisDocument2 pagesRRL in Thesismark_torreon100% (1)
- A. Subanen Elders' Interest in The Restoration of Subanen Language 2023Document12 pagesA. Subanen Elders' Interest in The Restoration of Subanen Language 2023MEDELYN INTONGNo ratings yet
- Shona Made Easy: Click To Edit Master Subtitle StyleDocument25 pagesShona Made Easy: Click To Edit Master Subtitle StyleInnocent Clifford Marandu100% (1)
- Early Aristocratic Seals: An Anglo-Norman Success Story : Jean-François NieusDocument25 pagesEarly Aristocratic Seals: An Anglo-Norman Success Story : Jean-François NieusIZ PrincipaNo ratings yet
- Medina Side Book Fiqh Level 2Document30 pagesMedina Side Book Fiqh Level 2Mountainofknowledge100% (2)
- Control Aveo1Document42 pagesControl Aveo1carlosNo ratings yet
- M.SC Maths (Previous)Document11 pagesM.SC Maths (Previous)hari sharmaNo ratings yet
- RA 7942 Plus CasesDocument53 pagesRA 7942 Plus CasesJessielleNo ratings yet
- Tapta MudradharaneDocument2 pagesTapta MudradharanenaraharisumadhwaNo ratings yet
- Australian Magpies Gymnorhina Tibicen Cooperate To Remove Tracking DevicesDocument5 pagesAustralian Magpies Gymnorhina Tibicen Cooperate To Remove Tracking Deviceswds657No ratings yet
- Atty Paras Reprimanded for Delayed ComplianceDocument10 pagesAtty Paras Reprimanded for Delayed ComplianceMK KMNo ratings yet
- Summer Internship Project Report ON "Apple V/S Samsung": Sardar Bhagat Singh College of Technology & Management, LucknowDocument4 pagesSummer Internship Project Report ON "Apple V/S Samsung": Sardar Bhagat Singh College of Technology & Management, LucknowMaster PrintersNo ratings yet
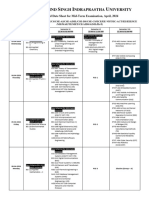
- Mid Term Date Sheet - pq0NsApDocument2 pagesMid Term Date Sheet - pq0NsApSahil HansNo ratings yet
- School Management Assessment ToolDocument24 pagesSchool Management Assessment ToolMa Abegail Calayag Carangan100% (7)
- ROLAND SolJet Pro 4 XR 640 Service Manual Direct DownloadDocument271 pagesROLAND SolJet Pro 4 XR 640 Service Manual Direct DownloadZevnik d.o.o.100% (1)
- Learn Steel 2007 Limit State Design of Structural Steel MembersDocument31 pagesLearn Steel 2007 Limit State Design of Structural Steel MembersshaikcivilNo ratings yet
- Mapping and Analysis of Efforts To Counter Information Pollution PDFDocument48 pagesMapping and Analysis of Efforts To Counter Information Pollution PDFAhmad Ridzalman JamalNo ratings yet