Professional Documents
Culture Documents
COMUNICAZ. 07 - Lancet Paper
Uploaded by
ハルァン ファ烏山0 ratings0% found this document useful (0 votes)
27 views12 pagesMedical
Copyright
© © All Rights Reserved
Available Formats
PDF, TXT or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentMedical
Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
0 ratings0% found this document useful (0 votes)
27 views12 pagesCOMUNICAZ. 07 - Lancet Paper
Uploaded by
ハルァン ファ烏山Medical
Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
You are on page 1of 12
Seminar
234 www.thelancet.com Vol 372 July 19, 2008
Polymyalgia rheumatica and giant-cell arteritis
Carlo Salvarani, Fabrizio Cantini, Gene G Hunder
Polymyalgia rheumatica and giant-cell arteritis are closely related disorders that aect people of middle age and older.
They frequently occur together. Both are syndromes of unknown cause, but genetic and environmental factors might
have a role in their pathogenesis. The symptoms of polymyalgia rheumatica seem to be related to synovitis of proximal
joints and extra-articular synovial structures. Giant-cell arteritis primarily aects the aorta and its extracranial
branches. The clinical ndings in giant-cell arteritis are broad, but commonly include visual loss, headache, scalp
tenderness, jaw claudication, cerebrovascular accidents, aortic arch syndrome, thoracic aorta aneurysm, and
dissection. Glucocorticosteroids are the cornerstone of treatment of both polymyalgia rheumatica and giant-cell
arteritis. Some patients have a chronic course and might need glucocorticosteroids for several years. Adverse events
of glucocorticosteroids aect more than 50% of patients. Trials of steroid-sparing drugs have yielded conicting
results. A greater understanding of the molecular mechanisms involved in the pathogenesis should provide new
targets for therapy.
Denitions and diagnostic criteria
Giant-cell arteritis mainly involves the large and
medium-sized arteries, especially branches of the
proximal aorta. Polymyalgia rheumatica is characterised
by aching and morning stiness in the shoulder and
pelvic girdles and neck. The two disorders can occur
separately or together in people aged 50 years and older.
The diagnosis of polymyalgia rheumatica depends on a
combination of clinical symptoms, raised acute-phase
reactants, exclusion of other diseases, and response to
glucocorticosteroids. At least three sets of diagnostic
criteria for polymyalgia rheumatica are used in clinical
practice (panel).
13
The criteria formulated by Chuang and
co-workers
1
and by Healey,
2
on the basis of clinical
experience, are much the same. The core symptoms are
proximal pain and stiness; the only dierence is the
inclusion in the Healey criteria of the response to
glucocorticosteroids.
Criteria for the classication of giant-cell arteritis were
developed by the American College of Rheumatology
in 1990 (table).
4
These criteria were designed to
dierentiate this disease from other vasculitides, and are
not useful for making the diagnosis in individual
patients.
5
Temporal artery biopsy remains the gold
standard for diagnosis of giant-cell arteritis. Because of
skip inammatory lesions, specimen length should be at
least of 153 cm, to keep false negative results to a
minimum.
6
Routine examination of temporal artery
biopsy at multiple levels does not substantially increase
the diagnostic yield.
7
Since negative unilateral temporal
artery biopsy is associated with an extremely low
frequency (13%) of subsequent positive contralateral
biopsy, bilateral biopsy is not recommended as an initial
routine procedure.
8,9
When possible, temporal artery biopsy should be done
before treatment is started; however, specimens might
show arteritis after more than 2 weeks of
glucocorticosteroid therapy.
10
Achkar and colleagues
10
showed that in a consecutive cohort of 535 patients who
had temporal artery biopsies, the positivity rates of
temporal artery biopsy were similar in untreated and
corticosteroids treated patients (31% vs 35%). Studies
have assessed possible predictors of positive temporal
artery biopsy. The combination of jaw claudication plus
double vision predicted a positive biopsy in all patients in
one study, whereas a normal ESR before treatment made
giant-cell arteritis unlikely, but it does not exclude
completely this diagnosis.
11,12
Epidemiology
The incidence rates of giant-cell arteritis and polymyalgia
rheumatica increase progressively after 50 years of age.
13
The reported rates for giant-cell arteritis are highest in
northern European countries and in Minnesota (USA),
which has a population of similar ethnic background, and
are 20 or more per 100 000 people older than 50 years.
1416
Rates of this disease are lower in Mediterranean
countries
17,18
and lowest in Arabian and Asian countries.
19,20
The lowest prevalence was reported in Japan (147 per
100 000 population older than 50 years).
20
Autopsy studies
suggest that giant-cell arteritis might be more common
than is clinically apparent.
21
Women are aected two to three times more commonly
than are men. The incidence of giant-cell arteritis has
increased over the past 2040 years, possibly because of
increased awareness. Some studies have reported
seasonal variations or a cyclic pattern.
22,23
Although
Lancet 2008; 372: 23445
Unit of Rheumatology,
Arcispedale S Maria Nuova,
Reggio Emilia, Italy
(C Salvarani MD); Unit of
Rheumatology, Division of
Medicine, Ospedale di Prato,
Prato, Italy (F Cantini MD); and
Mayo Clinic College of
Medicine, Rochester, MN, USA
(G G Hunder MD)
Correspondence to:
Dr Carlo Salvarani, Unit of
Rheumatology, Arcispedale
S Maria Nuova, V.le Risorgimento
N80, 42100 Reggio Emilia, Italy
salvarani.carlo@asmn.re.it
Search strategy and selection criteria
We searched the Cochrane Library, Medline, and EMBASE,
mainly using the search terms polymyalgia rheumatica
[Mesh], giant cell arteritis [Mesh], and temporal arteritis
[Mesh]. We largely selected articles published in English
during the past 5 years, without excluding older papers that
we considered to be highly relevant to the topics discussed in
this Seminar. We also searched the reference lists of articles
identied by this search strategy, and selected those that we
judged relevant. We also included some review papers
providing insightful overviews on polymyalgia rheumatica
and giant-cell arteritis.
Seminar
www.thelancet.com Vol 372 July 19, 2008 235
patients with this disease have an increased risk of
developing aortic aneurysm and dissection, and
cerebrovascular accidents, most studies of long-term
survival have shown no excess mortality.
24
Polymyalgia rheumatica is two to three times more
common than is giant-cell arteritis, although the
distribution is similar.
16,17,2527
In Olmsted County,
Minnesota, the average yearly incidence was 525 cases
per 100 000 people aged 50 years and older.
25
Population-based studies have shown a fairly stable
incidence of polymyalgia rheumatica in recent years.
Relation between giant-cell arteritis and
polymyalgia rheumatica
The clinical connections between polymyalgia rheumatica
and giant-cell arteritis have suggested that they are
dierent manifestations of the same disease process.
These connections include their frequent occurrence
together, the older age at onset with progressively
increasing incidence rates after 50 years, similar sex ratio,
substantial increase of acute-phase reactants before
treatment, and rapid responsiveness to glucocortico-
steroids and outcome.
13
Population-based studies have
shown that 1621% of patients with polymyalgia
rheumatica have giant-cell arteritis, and polymyalgia
rheumatica is present in 4060% of patients with giant-cell
arteritis.
22,25,26
Polymyalgia rheumatica might begin before,
appear simultaneously with, or develop after clinical
manifestations of giant-cell arteritis. A few patients with
polymyalgia rheumatica without ndings of giant-cell
arteritis at diagnosis have a positive temporal artery biopsy
or develop giant-cell arteritis during follow-up.
28,29
PET-
evidence of vascular uorodeoxyglucose uptake,
predominantly at subclavian arteries, was noted in 30% of
patients with isolated polymyalgia rheumatica at
diagnosis,
30
despite a negative biopsy sample of temporal
artery.
This study conrms that most patients with isolated
polymyalgia rheumatica do not have evidence of vasculitis;
however large artery vasculitis may be present in
polymyalgia rheumatica even in absence of temporal
arteries involvement.
Pathology and pathogenesis
In giant-cell arteritis, inammation mainly aects the
large and medium-sized muscular arteries, especially the
proximal aorta and its branches.
13,31
These arteries have a
prominent internal elastic membrane and vasa vasorum.
As the cervical arteries penetrate the dura they become
thinner, have much less elastic tissue, and no vasa
vasorum. Intracranial arteries are rarely associated with
the vasculitic process.
32
The classic histological picture of giant-cell arteritis is
characterised by a granulomatous inammatory inltrate
with lymphocytes, macrophages, and multinucleated
giant cells, which are usually located at the intima-media
junction (gure 1). However, only about 50% of routine
biopsy samples show all these typical features. The others
manifest a chronic inammatory reaction, featuring
lymphomononuclear cells and sparse neutrophils and
eosinophils, but no giant cells (gure 1). Inammation
tends to aect the arteries in a segmental fashion, and the
inammatory process is usually most severe in the inner
portion of the media adjacent to the disrupted internal
elastic lamina.
33,34
In some cases the inammation is
restricted to the vasa vasorum or to periadventitial small
vessels, or both (gure 1).
35
In such instances, the diagnosis
of giant-cell arteritis might not be straightforward.
Denition
Age at disease onset 50 years Development of symptoms or ndings beginning at 50 years or older
New headache New onset of or new type of localised pain in the head
Temporal artery abnormality Temporal artery tenderness to palpation or decreased pulsation, unrelated
to arteriosclerosis of cervical arteries
Increased ESR ESR 50 mm/h by the Westergren method
Abnormal artery biopsy Biopsy specimen with artery showing vasculitis characterised by a
predominance of mononuclear cell inltration or granulomatous
inammation, usually with multinucleated giant cells
*For purposes of classication, a patient with vasculitis is said to have giant-cell (temporal) arteritis if at least three of
these ve criteria are present. The presence of any three or more criteria yields a sensitivity of 935% and a specicity
of 912%. Adapted from reference 4.
Table: 1990 criteria for the classication of giant-cell (temporal) arteritis (traditional format)*
Panel: Diagnostic criteria for polymyalgia rheumatica
Chuang et al
1
1 Patients 50 years or older
2 Bilateral aching and stiness persisting for 1 month or more involving two of the
following areas: neck or torso, shoulders or proximal regions of the arms, and hips or
proximal aspects of the thighs
3 ESR greater than 40 mm/h
4 Exclusion of other diagnoses except giant-cell arteritis
The presence of all these criteria denes diagnosis of polymyalgia rheumatica.
Healey
2
1 Persistent pain (for at least 1 month) involving two of the following areas: neck,
shoulders, and pelvic girdle
2 Morning stiness lasting more than 1 h
3 Rapid response to prednisone (20 mg/day)
4 Absence of other diseases capable of causing the musculoskeletal symptoms
5 Age over 50 years
6 ESR greater than 40 mm/h
The diagnosis of polymyalgia rheumatica is made if all the above criteria are satised.
Bird
3
1 Bilateral shoulder pain and/or stiness
2 Onset of illness within 2 weeks
3 Initial ESR higher than 40 mm/h
4 Morning stiness exceeding 1 h
5 Age older than 65 years
6 Depression and/or loss of weight
7 Bilateral upper arm tenderness
A diagnosis of probable polymyalgia rheumatica is made if any three or more of these
criteria are fullled. The presence of any three or more criteria yields a sensitivity of 92%
and a specicity of 80%.
Seminar
236 www.thelancet.com Vol 372 July 19, 2008
In polymyalgia rheumatica, pathological ndings are
much less prominent than they are in giant-cell arteritis.
A mild synovitis characterised by a predominance of
macrophages and CD4+ T-lymphocytes has been described
in specimens of shoulder synovial membranes and other
involved joints.
36
The cause of both disorders remains unknown. Their
decreasing incidence with a northsouth gradientthe
highest incidence being in Scandinavian countries and
in US communities with a Scandinavian ethnic
backgroundand the occasional familial cases lend
support to a role for both environmental and genetic
risk factors.
1416,25,26
The cyclic pattern of yearly incidence
rates and the seasonal variations reported by some
studies might suggest an environmental-infectious
aetiology.
22,23,37
Several viruses have been investigated as
possible triggers in a susceptible host, with inconclusive
results.
38
With regard to cardiovascular risk factors,
casecontrol studies have reported an increased risk of
giant-cell arteritis in heavy smokers, and in patients
with previous atherosclerotic disease.
3941
A wide variety of immunogenetic factors have been
studied in giant-cell arteritis and polymyalgia rheumatica.
In patients with giant-cell arteritis, the most commonly
identied genetic association is with HLA-DRB1*04
alleles. However, the strength of the HLA-DRB1
association with polymyalgia rheumatica varies between
dierent populations.
17,42,43
Knowledge of mechanisms of the inammation has
advanced in recent years. Weyand and Goronzy
44
and
co-workers
45
have suggested that dendritic cells located at
the adventitia-media border of the artery have a crucial
role in initiation of vasculitis. The dendritic cells in the
wall can be activated by toll-like receptor ligands (or
perhaps an unknown antigen entering via the vasa
vasorum). The activated dendritic cells become
chemokine-producing eector cells, which recruit CD4
T-cells into the vascular wall through the vasa vasorum.
Macrophages are also recruited. The activated dendritic
cells provide the necessary costimulatory signals to
trigger T-cell activation. The recruited and activated CD4+
T cells in the artery wall undergo clonal expansion and
begin secreting cytokines including interferon-, which
has a pivotal part in regulation of the dierentiation and
function of macrophages. In the adventitia, macrophages
produce the inammatory cytokines interleukin 1 and
interleukin 6, whereas in the media they release
metalloproteinases and reactive oxygen intermediates.
These inammatory mediators lead to the fragmentation
of the internal elastic lamina and trigger repair
mechanisms such as intimal hyperplasia and
neoangiogenesis, which are regulated by platelet-derived
growth factor and vascular endothelial growth factor.
Platelet-derived growth factor seems to be crucial in
induction of intimal hyperplasia and vessel occlusion.
46
In patients with polymyalgia rheumatica who do not
have histological evidence of arteritis, adventitial
dendritic cells are in an activated state, and both
interleukin 1 and interleukin 6 are detectable in the
so-called histologically normal temporal arteries.
However, interferon--producing T cells are not recruited
into vascular tissue. Without interferon-, arterial
inammation in polymyalgia rheumatica remains
Ref number
Editor
Author
Created by
Section
Text retyped
Image redrawn
Special Characters Palette
Urgent
Special instructions
$
+<>
07tl6309_1
Editor name: HC
Author name
Illustrator name
Section name
Tick Marks
Axis break Error bar
Shaker 65 roman
Subscript
123456789
Superscript
1 2 3 4 5 6 7 8 9
Superiors (GLYPHS) Inferiors
Key 1
Key 2
Key 3
Key 4
Key 5
Key 1
Key 2
Key 3
Key 4
Key 5
Key 4
Key 5
Key 4
Key 5
D
E F
G H
I J
K L
Shaker 85 bold
A B
C
A
B
C
Figure 1: Histopathological features of giant-cell arteritis
Transverse sections of temporal artery from patients with untreated giant-cell
arteritis are shown. (A) Granulomatous inammation and multinucleated giant
cells (arrows) at junction of media and intima (haematoxylin and eosin, 100).
(B) A mononuclear transmural inltrate without giant cells (haematoxylin and
eosin, 40). (C) Vasculitis involving small vessels (arrows) close to a
non-inamed temporal artery (haematoxylin and eosin, 40).
Seminar
www.thelancet.com Vol 372 July 19, 2008 237
subclinical.
47
The systemic manifestations of giant-cell
arteritis and polymyalgia rheumatica are caused by the
production of inammatory cytokines derived from
macrophages. Several studies have suggested that
patients with a lower inammatory response have a
higher risk of developing ischaemic manifestations than
do other patients.
48,49
Interleukin 6 expression in the
temporal artery, circulating concentrations of inter-
leukin 6, and angiogenic response are substantially
decreased in this subset of patients.
49,50
Angiogenic
activity of interleukin 6 might be an important protective
mechanism for ischaemia in giant-cell arteritis.
Clinical manifestations
Polymyalgia rheumatica
Polymyalgia rheumatica is typically characterised by aching
and stiness in the morning in the neck, shoulder, and
pelvic girdles. Typically the stiness in the morning lasts
30 min or more. Shoulder pain is the presenting nding in
7095% of patients, whereas hips and neck are less
frequently involved (5070%). The pain usually radiates
distally towards the elbows and knees. It can begin in one
shoulder or hip, but soon becomes bilateral. Occasionally
the symptoms begin more peripherally. Pain is most severe
with movement, and interferes with sleep at night. On
examination, painful restriction of active and often passive
movements of the shoulders and hips is present, without
detectable proximal joint swelling. Systemic signs and
symptoms such as low-grade fever, depression, fatigue,
anorexia, and weight loss occur in up to 40% of patients.
1,51
High, spiking fevers are uncommon in polymyalgia
rheumatica in the absence of giant-cell arteritis.
52,53
Distal musculoskeletal manifestations are seen in
about half of patients.
5455
They include carpal tunnel
syndrome; non-erosive, self-limited, asymmetric peri-
pheral arthritis (predominantly aecting the knees and
wrists); and diuse distal extremity swelling with pitting
oedema mostly over the dorsum of the hands and wrists,
but also over the ankles and tops of the feet.
Giant-cell arteritis
One or more systemic manifestations, including fever,
malaise, anorexia, and weight loss, are present in most
patients.
51,57
Fever is usually low grade, but it reaches
3940C in about 15% of patients and might be the
presenting manifestation or the only feature of giant-cell
arteritis.
52,53
A new-onset headache is the most frequent symptom,
occurring in two thirds of patients.
51,58
Head pain is
usually over the temporal or occipital areas, but it may
localise to any part of the head. Pain is usually continuous
throughout the day, often interferes with sleep, and
responds incompletely to analgesics. Nearly half of
patients suer from jaw claudication, due to ischaemia
of the muscles of mastication.
57
Jaw claudication is a high
predictor of giant-cell arteritis, but is not pathognomonic.
59
Occasionally, intermittent claudication can aect the
arms, tongue, or the muscles involved in swallowing.
On physical examination, the frontal or parietal
branches of the supercial temporal arteries may be
thickened, nodular, tender, or occasionally red. Pulses
may be decreased or absent. Scalp tenderness arises in
around half of patients; it is usually worsened by brushing
or combing the hair. It is seen most often in patients with
headaches.
Permanent partial or complete loss of vision in one or
both eyes occurs in less than 20% of patients, and is
often an early manifestation.
48,60,61
Visual loss is related to
anterior ischaemic optic neuropathy, which is caused
most commonly by narrowing or occlusion of the
posterior ciliary arteries. Less commonly, visual loss is
caused by retinal artery occlusion. The early fundoscopic
appearance noted in anterior ischaemic optic neuropathy
consists of slight pallor and oedema of the optic disc,
with scattered cotton-wool patches and small
haemorrhages (gure 2). Later, optic atrophy occurs
(gure 2). Patients who are aected typically report a
feeling of a shade covering one eye, which can progress
to total blindness. The eye is not painful. If untreated,
the second eye is likely to become aected within
12 weeks. Once visual impairment is established, it is
usually permanent. Amaurosis fugax is reported in
1015% of patients, and can precede permanent visual
loss. Transient diplopia is present in around 6% of
patients.
Polymyalgia rheumatica is the most frequent
musculoskeletal manifestation in giant-cell arteritis,
occurring in around 40% of patients. Distal symptoms,
such as peripheral arthritis and distal swelling with
pitting oedema, can arise in 25% of patients.
62
Less frequent onset patterns of polymyalgia rheumatica
and giant-cell arteritis
The diagnosis of polymyalgia rheumatica and giant-cell
arteritis is straightforward in patients with typical features.
However, both disorders are characterised by a wide range
of clinical manifestations, and can present with atypical
features, resulting in a challenging diagnosis.
Ref number
Editor
Author
Created by
Section
Text retyped
Image redrawn
Special Characters Palette
Urgent
Special instructions
$
+<>
07tl6309_2
Editor name: HC
Author name
Illustrator name
Section name
Tick Marks
Axis break Error bar
Shaker 65 roman
Subscript
123456789
Superscript
1 2 3 4 5 6 7 8 9
Superiors (GLYPHS) Inferiors
Key 1
Key 2
Key 3
Key 4
Key 5
Key 1
Key 2
Key 3
Key 4
Key 5
Key 4
Key 5
Key 4
Key 5
D
E F
G H
I J
K L
Shaker 85 bold
A B
C
A B
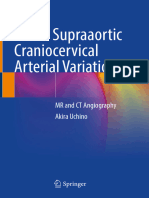
Figure 2: Photographs of the optic disc in patients with giant-cell arteritis and visual loss due to anterior
ischemic optic neuropathy, in the early acute phase (A) and after 3 months of prednisone therapy (B)
(A) Optic disc oedema and a ame-shaped haemorrhage is shown. (B) Optic atrophy is shown.
Seminar
238 www.thelancet.com Vol 372 July 19, 2008
Swelling and pitting oedema of the hands and feet
similar to that seen in patients with remitting
seronegative, symmetric synovitis with pitting oedema
syndrome are present in 812% of patients with
polymyalgia rheumatica.
5456
These ndings are frequently
unilateral in patients with polymyalgia rheumatica,
usually aect the dorsum of the hands and, less
frequently, of the feet and promptly remit after small
doses of corticosteroids. MRI shows that a substantial
tenosynovitis is the underlying lesion.
63
When these
distal ndings occur in elderly people, polymyalgia
rheumatica might represent the cause, and clinicians
should be alerted to investigate other signs and symptoms
of this disease.
Recent studies report a positive temporal artery biopsy
in only 139% of patients with polymyalgia rheumatica
without clinical features of giant-cell arteritis, compared
with the 1520% that was reported in earlier studies.
1,28,64
A high ESR and the presence of systemic manifestations
are predictors of coexistent silent giant-cell arteritis in
polymyalgia rheumatica. Patients with polymyalgia
rheumatica with silent giant-cell arteritis do not develop
ischaemic complications; therefore, temporal artery
biopsy is not indicated in patients with polymyalgia
rheumatica in the absence of cranial manifestations,
unless a high inammatory response is present.
Up to 15% of patients with giant-cell arteritis present
with fever of unknown origin.
52
Fever can reach 3940C,
and dominate the clinical picture. Shaking, rigors, and
sweats mimic sepsis. Giant-cell arteritis is responsible
for only 2% of all cases of fever of unknown origin, but of
up to 16% in patients older than 65 years.
52
In such cases,
a careful examination of the temporal arteries is indicated
and, if other disorders are excluded, a temporal artery
biopsy should be considered.
Ocular involvement may represent the presenting
manifestation of an otherwise clinically silent giant-cell
arteritis. In one prospective study,
65
21% of patients with
this disease and visual loss did not have other cranial or
systemic manifestations at disease onset. Giant cell
arteritis should be suspected when patients older than
50 years present with visual loss caused by anterior
ischaemic optic neuropathy or (less commonly) occlusion
of the central retinal artery, particularly when raised ESR
values are present.
Aortic arch syndrome occurs in about 1015% of
patients, presenting with claudication of the arms;
bruits over the carotid, subclavian, axillary and brachial
arteries; and absent or decreased pulses in the neck or
arms.
66,67
Large artery involvement in giant-cell arteritis
can also aect the legs.
68
Thoracic aortic aneurysms and
dissection of the aorta are important late complications
of giant-cell arteritis. Aneurysms tend to arise several
years after the diagnosis, and when other symptoms
have subsided.
66,67
Thoracic aortic aneurysms are
17 times more frequent in patients with giant-cell
arteritis than in non-aected people. A chest radiograph
every year is adequate to screen for thoracic aortic
aneurysm.
Neurological manifestations occur in about 30% of
patients.
69
In around 14% of all patients they consist of
neuropathies, including mononeuropathies and peripheral
polyneuropathies of the upper or lower extremities.
70
Less
common (34%) are transient ischaemic attacks, and
strokes caused by severe obstruction or occlusion of the
internal carotid or vertebral arteries.
69,71
Inammation of
intracranial or intradural arteries is very rare.
32
Respiratory tract symptoms including cough, sore throat,
and hoarseness occur in about 10% of patients.
72
When
these symptoms are prominent or an initial manifestation,
the diagnosis of giant-cell arteritis can be delayed.
Scalp necrosis, ulceration or infarction of the tongue,
pericardial and pleural eusions,
73
myocardial
infarctions,
74
female genital tract or breast involvement,
75,76
syndrome of inappropriate antidiuretic secretion,
77
and
dysarthria
78
are rare presentations of giant-cell arteritis.
Laboratory ndings and imaging
Laboratory ndings in both polymyalgia rheumatica and
giant-cell arteritis are non-specic but indicate the
inammatory nature of these syndromes. An ESR of at
least 40 mm/h has been included in all sets of criteria for
the diagnosis of polymyalgia rheumatica.
13
However, a
Ref number
Editor
Author
Created by
Section
Text retyped
Image redrawn
Special Characters Palette
Urgent
Special instructions
$
+<>
07tl6309_3
Editor name: HC
Author name
Illustrator name
Section name
Tick Marks
Axis break Error bar
Shaker 65 roman
Subscript
123456789
Superscript
1 2 3 4 5 6 7 8 9
Superiors (GLYPHS) Inferiors
Key 1
Key 2
Key 3
Key 4
Key 5
Key 1
Key 2
Key 3
Key 4
Key 5
Key 4
Key 5
Key 4
Key 5
D
E F
G H
I J
K L
Shaker 85 bold
A B
C
A
B
C
Figure 3: Ultrasonography (A) and MRI (B) of the shoulder, and uorodeoxyglucose-positron emission
tomography (C) of patients with isolated (absence of signs or symptoms of giant-cell arteritis) untreated
polymyalgia rheumatica
(A) Ultrasonography shows the presence of uid within the subacromial bursa (arrows) and surrounding the long
biceps tendon groove (arrowheads). (B) An axial T2 weighted section shows subacromial and subdeltoid bursitis
(pentagon), joint eusion (arrow), and tenosynovitis of the long head of the biceps (arrowhead).
(C) Fluorodeoxyglucose-positron emission tomography shows inammatory uorodeoxyglucose uptake in the
shoulders (arrows) and absence of vascular uptake.
Seminar
www.thelancet.com Vol 372 July 19, 2008 239
normal ESR has been reported in 720% of the patients
with polymyalgia rheumatica.
79
The American College of
Rheumatology classication criteria for giant-cell arteritis
include an ESR of 50 mm/h or more.
4
However, an ESR
less than 40 mm/h has been noted in 54% of patients,
and less than 50 mm/h in 108%.
80
Therefore, a normal
ESR does not exclude polymyalgia rheumatica or
giant-cell arteritis, particularly when other clinical
ndings suggest these diagnoses.
C-reactive protein is not as aected by extraneous
factors as the ESR, so is a more sensitive indicator of
disease activity in both disorders.
79,81
The ESR is a time
honoured laboratory parameter in both diseases, and we
suspect its use will continue. Some data indicate that
blood concentrations of interleukin 6 are the most
sensitive indicators of disease activity and course;
82,83
however, the test is not readily available in most
laboratories. Tests for rheumatoid factor and for
anticyclic citrullinated peptide antibodies are usually
negative.
84
A moderate anaemia of chronic disease (ie,
normocytic anaemia) is present in most patients, and
concentrations of liver enzymesparticularly alkaline
phosphataseare mildly raised in roughly a third,
particularly in those with giant-cell arteritis that is
proven by biopsy.
Scintigraphy, MRI, ultrasonography, and uorode-
oxyglucose-positron emission tomography have been
used in polymyalgia rheumatica to detect synovitis in
proximal joints and periarticular structures and could
help with diagnosis.
30,8689
Bilateral subacromial-subdeltoid
bursitis and trochanteric bursitis are the most frequent
lesions, and are present in almost all patients with
polymyalgia rheumatica who have pain in shoulder and
pelvic girdles, respectively (gure 3 and gure 4).
Ultrasonography and MRI are equally eective in
conrmation of the presence of these lesions, with
sensitivities and specicities more than 90%.
88,89
Ultrasonographic evidence of bilateral shoulder bursitis
can lend support to the diagnosis of polymyalgia
rheumatica in patients with normal ESR.
90
Ultrasonography and high-resolution MRI are useful
adjunctive methods in diagnosis of giant-cell arteritis
9193
since they can show inammatory changes in temporal
arteries. A recent meta-analysis
92
has conrmed that a
hypoechoic halo around the lumen of temporal arteries
on ultrasonography has a high specicity for giant-cell
arteritis; however, its sensitivity is substantially lower
than is the specicity.
91,92
Bright enhancement (a sign of
mural inammation) of the temporal artery on
high-resolution contrast-enhanced MRI is also highly
specic for giant-cell arteritis.
93
Conventional angiography, CT, CT angiography, MRI,
MR angiography, and ultrasonography can document
large-vessel involvement in giant-cell artertitis.
94,95
Arteriography with several views can outline bilateral,
smooth, tapering stenoses, or occlusions of the
subclavian, axillary, and proximal brachial arteries.
Arteries in the legs are less frequently involved.
68,94
Ultrasonography shows stenoses or occlusions of large
vessels, or both, and also inammatory oedema of the
vessel wall (halo sign) (gure 5).
95
Vessel-wall oedema on
MRI can also indicate disease activity. The extent of the
examination is more restricted with MRI and
ultrasonography than with arteriography.
Ref number
Editor
Author
Created by
Section
Text retyped
Image redrawn
Special Characters Palette
Urgent
Special instructions
$
+<>
07tl6309_4
Editor name: HC
Author name
Illustrator name
Section name
Tick Marks
Axis break Error bar
Shaker 65 roman
Subscript
123456789
Superscript
1 2 3 4 5 6 7 8 9
Superiors (GLYPHS) Inferiors
Key 1
Key 2
Key 3
Key 4
Key 5
Key 1
Key 2
Key 3
Key 4
Key 5
Key 4
Key 5
Key 4
Key 5
D
E F
G H
I J
K L
Shaker 85 bold
A B
C
B
C A
Figure 4: Ultrasonography (A) and MRI (B) of the hip and uorodeoxyglucose-positron emission tomography
(C) of patients with isolated (absence of signs or symptoms of giant-cell arteritis) untreated polymyalgia
rheumatica
(A) Ultrasonography shows the presence of uid within the trochanteric bursa (surrounding white line and
arrows). (B) An axial T2 weighted section shows trochanteric bursitis (arrows) and joint eusion (arrowhead).
(C) Fluorodeoxyglucose-positron emission tomography shows inammatory uorodeoxyglucose uptake in the
hips (arrows) and absence of vascular uptake.
Ref number
Editor
Author
Created by
Section
Text retyped
Image redrawn
Special Characters Palette
Urgent
Special instructions
$
+<>
07tl6309_5
Editor name: HC
Author name
Illustrator name
Section name
Tick Marks
Axis break Error bar
Shaker 65 roman
Subscript
123456789
Superscript
1 2 3 4 5 6 7 8 9
Superiors (GLYPHS) Inferiors
Key 1
Key 2
Key 3
Key 4
Key 5
Key 1
Key 2
Key 3
Key 4
Key 5
Key 4
Key 5
Key 4
Key 5
D
E F
G H
I J
K L
Shaker 85 bold
A B
C
A B
Figure 5: Fluorodeoxyglucose-positron emission tomography (A) and colour-doppler ultrasonography of the
axillary artery (B) of a patient with large-vessel giant-cell arteritis presenting with fever of unknown origin
(A) Fluorodeoxyglucose-positron emission tomography shows increased tracer uptake in the axillary (arrowheads)
arteries and in the aorta (arrow). (B) Colour-Doppler ultrasonography of the left axillary artery of the same patient
shows vessel wall oedema (halo sign [dark area around the lumen of the vessel which is indicated by the dotted
line]). Both increased tracer uptake on positron emission tomography scan and the presence of a halo on
ultrasonography are consistent with active vessel wall inammation.
Seminar
240 www.thelancet.com Vol 372 July 19, 2008
Fluorodeoxyglucose-positron emission tomography
seems to be a promising method in the detection of occult
involvement of the aorta and large vessels in patients with
giant-cell arteritis, especially those presenting with fever
of unknown origin (gure 5). 83% of patients with
giant-cell arteritis have evidence of large-vessel
inammation at diagnosis that is conrmed by positron
emission tomography, although most patients do not
develop arterial stenosis, occlusion, or aneurysms.
96
Dierential diagnosis
Several disorders can mimic polymyalgia rheumatica.
97
Peripheral arthritis, particularly aecting both hands,
can pose a challenge in the distinction of polymyalgia
rheumatica from elderly-onset rheumatoid arthritis.
Pronounced symmetrical peripheral synovitis, positive
rheumatoid factor and anticyclic citrullinated peptide
antibodies, and the development of joint erosions and
extra-articular manifestations dierentiate rheumatoid
arthritis from polymyalgia rheumatica. Follow-up is
sometimes needed to establish the correct diagnosis.
84
Swelling and oedema of the hands and feet in
polymyalgia rheumatica is similar to that occurring in
patients with remitting seronegative, symmetric synovitis
with pitting oedema syndrome.
54,63,98
The similarities and
concurrence of the two disorders suggest that they might
constitute part of the same disease.
55
Late onset spondyloarthritis is characterised by
oligoarthritis; distal pitting oedema, mainly of the lower
limbs; restricted involvement of the axial skeleton;
constitutional symptoms (ie, fever, anorexia, weight loss),
and raised ESR.
99
Proximal symptoms similar to
polymyalgia rheumatica have also been described.
100
The
presence of other manifestations of spondyloarthritis,
such as peripheral enthesitis, dactylitis, anterior uveitis,
the association with HLA-B27, and radiological evidence
of sacroiliitis help dierentiate late onset spondyloarthritis
from polymyalgia rheumatica.
Polyarticular calcium pyrophosphate deposition disease
might also present with polymyalgic symptoms.
101
The
identication of calcium pyrophosphate dihydrate crystal
in the synovial uid or the typical radiographical ndings
accord with the diagnosis of calcium pyrophosphate
deposition disease.
Patients with bromyalgia are usually younger than
are those with other disorders, do not have typical joint
stiness in the morning, and have normal acute-phase
reactants. Proximal muscular weakness rather than
pain, increased muscle enzyme concentrations, and
myopathic electromyographic changes distinguish
polymyositis from polymyalgia rheumatica.
102
Musculoskeletal aching in some malignancies and
infections can mimic polymyalgia rheumatica.
97,103,104
The
presence of more diuse pain, absent or minimal joint
stiness in the morning, little if any proximal joint
restriction, and absence of adequate response to
prednisone, should suggest further investigations.
However, no association exists between polymyalgia
rheumatica and malignancies. Other vasculitides can
also aect the temporal artery such as Wegeners
granulomatosis and polyarteritis nodosa. The
involvement of respiratory tract or kidney (or both), the
histopathology, and the presence of antineutrophil
cytoplasmic antibodies dierentiate these vasculitides
from giant-cell arteritis. Takayasus arteritis aects the
aorta and its major branches, but starts at an earlier age.
Primary vasculitis of the CNS aects only intracranial
arteries.
Treatment and course
Giant-cell arteritis
Glucocorticoids are the treatment of choice. Adequate
doses quickly suppress clinical manifestations of this
disorder and prevent most further ischaemic
complications. If visual loss has occurred before start of
treatment, it is not usually reversed.
13,105,106
Glucocorticoid
therapy should be initiated as soon as the diagnosis of
giant-cell arteritis is established. We recommend an
initial dose of 4060 mg per day of prednisone (or
equivalent) as a single or divided dose.
13
If the patient
does not respond promptly, the dose should be increased.
Initial high-dose intravenous methylprednisolone
(1000 mg every day for 3 days) can be tried in patients
with recent visual loss, although no documentation
suggests that it helps more than oral prednisone. A small
randomised controlled trial showed that intravenous
pulse methylprednisolone (15 mg/kg per day for 3 days)
given at onset of treatment allowed more rapid tapering
of the glucocorticoid dose over the ensuing weeks, and
resulted in a higher frequency of discontinuation of oral
glucocorticoid therapy, than did oral prednisone,
107
but a
larger trial which used pulse glucocorticoid therapy at a
lower dose did not show an additional benet over oral
glucocorticoids.
108
Treatment with alternate-day glucocorticoid
administration has been proposed to reduce the risk of
adverse reactions related to glucocorticoids, but is
associated with a higher rate of treatment failure than
daily administration (70% vs 20%),
109
and is not
recommended.
The initial dose of glucocorticoids is usually given for
24 weeks until all reversible signs and symptoms have
resolved and acute phase reactants are back to normal.
Then, the dose can be gradually reduced each week or
every 2 weeks by a maximum of 10% of the total daily
dose. The necessary duration of glucocorticoid therapy is
variable, but in most cases it can be discontinued within
12 years. Some patients have a chronic relapsing course
and might need low doses of glucocorticoids for several
years.
51,110,111
Even with gradual reduction of doses of
glucocorticoids, clinical ares have been reported to
occur in more than 50% of patients, particularly during
the rst 1216 months, when the prednisone dose is
reduced to about 510 mg per day.
111113
Seminar
www.thelancet.com Vol 372 July 19, 2008 241
The decision to reduce glucocorticoids should be based
on the regular assessment of clinical symptoms and
signs, and the ESR or concentration of C-reactive protein.
An isolated increased ESR is not usually a valid reason to
raise the dose. Some evidence suggests that interleukin 6
might be more sensitive than ESR and CRP for detection
of a disease-related, acute phase response and therefore
be a better predictor of disease are.
114
Adverse events related to glucocorticoids are common,
and are related to the age of patients and the cumulative
dose of glucocorticoids. In a population-based study,
111
86% of patients with giant-cell arteritis had adverse
events including bone fractures, avascular necrosis of the
hip, diabetes mellitus, infections, gastrointestinal
bleeding, cataract, and hypertensions.
111
Calcium
(10001500 mg per day) and vitamin D (800 IU per day)
should be given to all patients who take glucocorticoids.
Bisphosphonates are suggested for patients with
abnormal bone-mineral density (T score less than 1 SD).
Bone-mineral density at lumbar spine and hip should be
done when patients are starting glucocorticoids or soon
afterwards. If normal, bone-mineral density should be
repeated after 12 months of glucocorticoid treatment.
115,116
Three recent randomised controlled trials
112,113,117
have
assessed the ecacy of methotrexate in recent-onset
giant-cell arteritis; however, these studies arrived at
dierent conclusions. A meta-analysis
118
of data from the
above trials reported that adjunctive methotrexate
treatment in doses of 7515 mg per week reduced the
risk of a rst relapse by 35%, and of a second relapse
by 51%. Additionally, adjunctive treatment with
methotrexate reduced the cumulative exposure to
glucocorticoids. However, the advantage of the treatment
eect of methotrexate compared with placebo fully
appeared only after 2436 weeks, and there was no
dierence between groups in the occurrence of adverse
events. We feel that methotrexate might be useful in
treatment of patients at high risk of side-eects related
to glucocorticoids for comorbid conditions such as
diabetes mellitus, severe osteoporosis, and severe
hypertension, but not on a routine basis. Higher doses
of methotrexate (2025 mg per week) have not been
adequately studied.
Studies of azathioprine
119
and antitumour necrosis
factor (TNF)
120
have not shown a consequential eect.
However, a role for iniximab in patients with
glucocorticoid-refractory disease cannot be excluded.
121,122
Although ischaemic damage in giant-cell arteritis is not
usually attributed to thromboembolic occlusion, two
retrospective studies
123,124
have shown that aspirin use was
associated with a reduction of cranic ischaemic
complications of giant-cell arteritis. Experimental studies
lend support to these ndings.
125
Although a prospective
study is needed to dene the role of aspirin in giant-cell
arteritis, we recommend low-dose aspirin, in the absence
of specic contraindications, as an adjunctive drug in
this disease at diagnosis, together with a proton-pump
inhibitor because of the combined treatment with
glucocorticoids.
Polymyalgia rheumatica
An initial dose of 1020 mg per day of prednisone or
equivalent is adequate, in most cases, in the absence of
associated giant-cell arteritis.
126
Usually the response to
glucocorticoids is rapid, with complete or nearly
complete resolution of the musculoskeletal aching and
stiness within a few days. A few patients with isolated
polymyalgia rheumatica need a progressive dose increase
to 30 mg per day. The absence of improvement after
30 mg per day of prednisone for 1 week should alert the
physicians to question the diagnosis. After 23 weeks,
the daily dose can be reduced by 25 mg every 2 weeks to
10 mg per day. Subsequently, daily doses are reduced by
1025 mg every month until the treatment is
suspended. Two recent studies
83,127
reported a relapse
frequency of 50% in patients with polymyalgia
rheumatica. Increased initial doses of glucocorticoids
and faster tapering were substantial predictors of relapse,
so eorts should be made to keep the initial glucocorticoid
dose as low as possible, and to discontinue slowly.
The presence and degree of symptoms and an ESR or
C-reactive protein concentration can be used to monitor
the dose of glucocorticoids.
79
A treatment course of
12 years is often required. However, some patients
might need low doses of glucocorticoids for several
years.
51,128
Some studies have suggested that persistently
raised concentrations of C-reactive protein and
interleukin 6 are helpful in identication of patients with
relapsing disease.
82,83
About 65% of patients with polymyalgia rheumatica
have at least one serious event related to giant-cell
arteritis; in particular the risk of vertebral fractures is
ve times greater in women with polymyalgia
rheumatica. Older age at diagnosis, a cumulative dose
of prednisone of at least 2 g, and female sex independently
increased the risk of adverse events.
129
The measures
proposed to prevent or treat osteoporosis induced by
glucocorticoids should also be adhered to in polymyalgia
rheumatica.
115,116
Methotrexate has been proposed as a corticoid-sparing
drug in polymyalgia rheumatica with conicting results.
However, a recent randomised controlled trial
130
has
suggested that methotrexate can be eective in
polymyalgia rheumatica when the drug is started at
disease onset and given for at least 1 year at a dose of at
least 10 mg per week. This schedule can reduce the
incidence of ares and the amount of prednisone needed
to maintain remission.
Two pilot studies
131,132
reported that TNF-blocking agents
had a glucocorticoid-sparing eect in the treatment of
patients who are resistant to glucocorticoid therapy.
However, iniximab was ineective in a recent
randomised controlled trial of newly diagnosed
polymyalgia rheumatica.
133
Seminar
242 www.thelancet.com Vol 372 July 19, 2008
Future perspectives
The development of standardised classication and
diagnostic criteria would help in a comparison of studies
from dierent centres and assist clinicians. Additional
investigation is needed about the use of pulse
glucocorticoids at the onset of treatment for giant-cell
arteritis to conrm whether this regimen reduces toxic
eects of glucocorticoids. Identication of risk factors for
extended and relapsing disease might allow a more
eective use of glucocorticoids and could help in the
decision about the use of methotrexate. Randomised
controlled trials are needed to assess new therapeutic
agents. Strong evidence suggests that interleukin 6 has a
major role in sustaining disease activity in giant-cell
arteritis and polymyalgia rheumatica.
82,83,114
Therefore,
interleukin-6 inhibition with tocilizumab (humanised
anti-interlukin-6 receptor monoclonal antibody) might
be a logical target for future randmoised controlled
trials.
134
Other possible therapeutical agents include new
formulations of glucocorticosteroids and abatacept, a
recombinant fusion protein that modulates CD28-
mediated T-cell costimulation.
135
A better understanding of the molecular mechanisms
involved in the pathogenesis of polymyalgia rheumatica
and giant-cell arteritis should facilitate the development
of drugs that are able to inhibit selectively single
molecules or pathways that contribute to inammation.
Conict of interest statement
We declare that we have no conict of interest.
Acknowledgments
We thank Italo Portioli for his continuous support in the study of
polymyalgia rheumatica and giant-cell arteritis; GianLuigi Bajocchi,
Luigi Boiardi, Luca Cimino, PierLuigi Macchioni, Riccardo Meliconi,
Ignazio Olivieri, Nicol Pipitone, and Lia Pulsatelli for their
collaboration in patient care and in clinical studies on polymyalgia
rheumatica and giant-cell arteritis; Libero Barozzi and Giulio Zuccoli for
providing MRI documentation; Mauro Silingardi, Alberto Nicolini, and
Angelo Ghirarduzzi for providing US documentation; Annibale Versari
for his collaboration in positron emission tomography studies and for
provision of positron emission tomography images; and Alberto Cavazza
for providing histological documentation. This Seminar is dedicated to
the memory of Paolo Manganelli, a kind, soft spoken gentleman and
friend who was an outstanding clinician, teacher, and researcher.
References
1 Chuang T-Y, Hunder GG, Ilstrup DM, Kurland LT. Polymyalgia
rheumatica: a 10-year epidemiologic and clinical study.
Ann Intern Med 1982; 97: 67280.
2 Healey LA. Long-term follow-up of polymyalgia rheumatica:
evidencefor synovitis. Semin Arthritis Rheum 1984; 13: 32228.
3 Bird HA, Esselinckx W, Dixon ASJ, Mowat AG, Wood PHN. An
evaluation of criteria for polymyalgia rheumatica. Ann Rheum Dis
1979; 38: 43439.
4 Hunder GG, Bloch DA, Michel BA, et al. The American College of
Rheumatology 1990 criteria for the classication of giant cell
(temporal) arteritis. Arthritis Rheum 1990; 33: 112228.
5 Rao K, Allen NB, Pincus T. Limitations of the 1990 American
College of Rheumatology classication criteria in the diagnosis of
vasculitis. Ann Intern Med 1998; 129: 34552.
6 Taylor-Gjevre R, Vo M, Shukla D, Resch L. Temporal artery biopsy
for giant cell arteritis. J Rheumatol 2005; 32: 127982.
7 Chakrabarty A, Franks AJ. Temporal artery biopsy: is there any
value in examining biopsies at multiple levels? J Clin Pathol 2000;
53: 13136.
8 Boyev LR, Miller NR, Green WR. Ecacy of unilateral versus
bilateral temporal artery biopsies for the diagnosis of giant cell
arteritis. Am J Ophthalmol 1999; 128: 21115.
9 Hall JK, Volpe NJ, Galetta SL, Liu GT, Syed NA, Balcer LJ. The role
of unilateral temporal artery biopsy. Ophthalmology 2003;
110: 54348.
10 Achkar AA, Lie JT, Hunder GG, OFallon WM, Gabriel SE. How
does previous corticosteroid treatment aect the biopsy ndings in
giant cell (temporal) arteritis? Ann Intern Med 1994; 120: 98792.
11 Younge BR, Cook BE, Bartley GB, Hodge DO, Hunder GG.
Initiation of glucocorticoid therapy: before or after temporal artery
biopsy? Mayo Clin Proc 2004; 79: 48391.
12 Smetana GW, Shmerling RH. Does this patient have temporal
arteritis? JAMA 2002; 287: 92101.
13 Salvarani C, Cantini F, Boiardi L, Hunder GG. Polymyalgia
rheumatica and giant-cell arteritis. N Engl J Med 2002; 347: 26171.
14 Salvarani C, Crowson CS, OFallon WM, Hunder GG, Gabriel SE.
Reappraisal of the epidemiology of giant cell arteritis in Olmsted
County, Minnesota, over a fty-year period. Arthritis Rheum 2004;
51: 26468.
15 Nordborg E, Nordborg C. Giant cell arteritis: epidemiological clues
to its pathogenesis and an update on its treatment. Rheumatology
2003; 42: 41321.
16 Gran JT, Myklebust G. The incidence of polymyalgia rheumatica
and temporal arteritis in the county of Aust Agder, south Norway:
a prospective study 19871994. J Rheumatol 1997; 24: 173943.
17 Salvarani C, Macchioni PL, Zizzi F, et al. Epidemiologic and
immunogenetic aspects of polymyalgia rheumatica and giant cell
arteritis in Northern Italy. Arthritis Rheum 1991; 34: 35156.
18 Gonzalez-Gay MA, Miranda-Filloy JA, Lopez-Diaz MJ, et al. Giant
cell arteritis in Northwestern Spain. A 25-year epidemiologic study.
Medicine 2007; 86: 6168.
19 Chaudhry IA, Shamsi FA, Elzaridi E, Arat YO, Bosley TM, Riley FC.
Epidemiology of giant cell arteritis in an Arab population: a 22-year
study. Br J Ophthalmol 2007; 91: 71518.
20 Kobayashi S, Yano T, Matsumoto Y, et al. Clinical and epidemiologic
analysis of giant cell (temporal) arteritis from a nationwide survey
in 1998 in Japan: the rst government-supported nationwide survey.
Arthritis Rheum 2003; 49: 59498.
21 stberg G. On arteritis with special reference to polymyalgia
arteritica. Acta Pathol Microbiol Scand (A) 1973; 237 (suppl): 159.
22 Salvarani C, Gabriel SE, OFallon WM, Hunder GG. The incidence
of giant cell arteritis in Olmsted County, Minnesota: apparent
uctuations in a cyclic pattern. Ann Intern Med 1995; 123: 19294.
23 Bas-Lando M, Breuer GS, Berkun Y, Mates M, Sonnenblick M,
Nesher G. The incidence of giant cell arteritis in Jerusalem over a
25-year period: annual a seasonal uctuations. Clin Exp Rheumatol
2007; 25 (suppl 44): S1517.
24 Nuenningho DM, Hunder GG, Christianson TJH, McClelland RL,
Matteson EL. Mortality of large-artery complication (aortic
aneurysm, aortic dissection, and/or large-artery stenosis) in patients
with giant cell arteritis. A population-based study over 50 years.
Arthritis Rheum 2003; 48: 353237.
25 Salvarani C, Gabriel SE, OFallon WM, Hunder GG. Epidemiology
of polymyalgia rheumatica in Olmsted County, Minnesota,
19701991. Arthritis Rheum 1995; 38: 36973.
26 Franzn P, Sutinen S, Von Knorring J. Giant cell arteritis and
polymyalgia rheumatica in a region of Finland: an epidemiologic,
clinical and pathologic study, 1984-1988. J Rheumatol 1992; 19: 27380.
27 Smeeth L, Cook C, Hall AJ. Incidence of diagnosed polymyalgia
rheumatica and temporal arteritis in the United Kingdom,
1990-2001. Ann Rheum Dis 2006; 65: 109398.
28 Cantini F, Niccoli L, Storri L, et al. Are polymyalgia reumatica and
giant cell arteritis the same disease? Semin Arthrititis Rheum 2004;
33: 294301.
29 Gonzalez-Gay MA. Giant cell arteritis and polymyalgia rheumatica:
two dierent but often overlapping conditions.
Semin Arthritis Rheum 2004; 33: 28993.
30 Blockmans D, De Ceuninck L, Vanderschueren S, Knockaert D,
Mortelmans L, Bobbaers H. Repetitive 18-uorodeoxyglucose
positron emission tomography in isolated polymyalgia rheumatica:
a prospective study in 35 patients. Rheumatology (Oxford) 2007;
46: 67277.
Seminar
www.thelancet.com Vol 372 July 19, 2008 243
31 Wilkinson IMS, Russell RWR. Arteries of the head and neck in
giant cell arteritis. A pathological study to show the pattern of
arterial involvement. Arch Neurol 1972; 27: 37891.
32 Salvarani C, Giannini C, Miller DV, Hunder G. Giant cell arteritis:
involvement of intracranial arteries. Arthritis Rheum 2006; 55: 98589.
33 Lie JT. Illustrated histopathologic classication criteria for selected
vasculitis syndromes. Arthritis Rheum 1990; 33: 107487.
34 Klein RG, Campbell RJ, Hunder GG, Carney JA. Skip lesions in
temporal arteritis. Mayo Clin Proc 1976; 51: 50410.
35 Esteban M-J, Font C, Hernandez-Rodriguez J, et al. Small-vessel
vasculitis surrounding a spared temporal artery: clinical and
pathologic ndings in a series of twenty-eight patients.
Arthritis Rheum 2001; 44: 138795.
36 Meliconi R, Pulsatelli L, Uguccioni M, et al. Leukocyte inltration
in synovial tissue from the shoulder of patients with polymyalgia
rheumatica. Quantitative analysis and inuence of corticosteroid
treatment. Arthritis Rheum 1996; 39: 1199207.
37 Elling P, Olsson AT, Elling H. Synchronous variations of the
incidence of temporal arteritis and polymyalgia rheumatica in
dierent regions of Denmark; association with epidemics of
Mycoplasma pneumoniae infection. J Rheumatol 1996; 23: 11219.
38 Duhaut P, Bosshard S, Ducroix J-P. Is giant cell arteritis and
infectious disease? Biological and epidemiological evidence.
Presse Med 2004; 33: 140308.
39 Machado EBV, Gabriel SE, Beard CM, Michet CJ, OFallon WM,
Ballard DJ. A population-based case-control study of temporal
arteritis: evidence for an association between temporal arteritis and
degenerative vascular disease? Int J Epidemiol 1989; 18: 83641.
40 Duhaut P, Pinede L, Demolombe-Rague S, et al. Giant cell arteritis
and cardiovascular risk factors. A multicenter, prospective
case-control study. Arthritis Rheum 1998; 41: 196065.
41 Gonzalez-Gay MA, Pineiro A, Gomez-Gigirey A, et al. Inuence of
traditional risk factors of atherosclerosis in the development of
severe ischemic complications in giant cell arteritis. Medicine 2004;
83: 34247.
42 Salvarani C, Boiardi L, Mantovani V, et al. HLA-DRB1 alleles
associated with polymyalgia rheumatica in northern Italy:
correlation with disease severity. Ann Rheum Dis 1999; 58: 30308.
43 Gonzalez-Gay MA, Amoli MM, Garcia-Porrua C, Ollier WER.
Genetic markers of disease. Susceptibility and severity in giant cell
arteritis and polymyalgia rheumatica. Semin Arthritis Rheum 2003;
33: 3848.
44 Weyand CM, Goronzy JJ. Medium- and large-vessel vasculitis.
N Engl J Med 2003; 349: 16069.
45 Weyand CM, Wei M-A, Pryshchep O, Groschel S, Bernardino R,
Goronzy JJ. Vascular dendritic cells in giant cell arteritis.
Ann NY Acad Sci 2005; 1062: 195208
46 Lozano E, Segarra M, Garcia-Martinez A, Hernanadez-Rodriguez J,
Cid MC. Imatinib mesylate inhibits in vitro and ex vivo biologic
responses related to vascular occlusion in giant cell arteritis.
Ann Rheum Dis; published online June 21, 2007.
DOI:10.1136/ard.2007.070805.
47 Weyand CM, Hicok KC, Hunder GG, Goronzy JJ. Tissue cytokine
patterns in patients with polymyalgia rheumatica and giant cell
arteritis. Ann Intern Med 1994; 121: 48491.
48 Salvarani C, Cimino L, Macchioni PL, et al. Risk factors for visual
loss in an Italian population-based cohort of patients with giant cell
arteritis. Arthritis Rheum 2005; 53: 29397.
49 Hernandez-Rodriguez J, Segarra M, Vilardell C, et al. Elevated
production of interleukin-6 is associated with a lower incidence of
disease-related ischemic events in patients with giant cell arteritis:
angiogenic activity of interleukin-6 as a potential protective
mechanism. Circulation 2003; 107: 242834.
50 Cid MC, Hernandez-Rodriguez J, Esteban MJ, et al. Tissue and
serum angiogenic activity is associated with low prevalence of
ischemic complications in patients with giant cell arteritis.
Circulation 2002; 106: 166471.
51 Salvarani C, Macchioni PL, Tartoni PL, et al. et al. Polymyalgia
rheumatica and giant cell arteritis: a 5-year epidemiologic and
clinical study in Reggio Emilia, Italy. Clin Exp Rheumatol 1987;
5: 20515.
52 Calamia KT, Hunder GG. Giant cell arteritis (temporal arteritis)
presenting as fever of undetermined origin. Arthritis Rheum 1981;
24: 141418.
53 Gonzalez-Gay MA, Garcia-Porrua C, Amor-Dorado JC, Llorca J.
Fever in biopsy proven giant cell arteritis: clinical implications in a
dened population. Arthritis Rheum 2004; 51: 65255.
54 Salvarani C, Gabriel S, Hunder GG. Distal extremity swelling with
pitting edema in polymyalgia rheumatica: report of nineteen cases.
Arthritis Rheum 1996; 39: 7380.
55 Salvarani C, Cantini F, Olivieri I, Hunder GG. Polymyalgia
rheumatica: a disorder of extraarticular synovial structures?
J Rheumatol 1999; 26: 51721.
56 Salvarani C, Cantini F, Macchioni L, et al. Distal musculoskeletal
manifestations in polymyalgia rheumatica. A prospective follow-up
study. Arthritis Rheum 1998; 41: 122126.
57 Calamia KT, Hunder GG. Clinical manifestations of giant cell
(temporal) arteritis. Clin Rheum Dis 1980; 6: 389403.
58 Gonzalez-Gay MA, Barros S, Lopez-Diaz MJ, Garcia-Porrua C,
Sanchez-Andrade A, Llorca J. Giant cell arteriris: disease patterns of
clinical presentation in a series of 240 patients. Medicine (Baltimore)
2005; 84: 26976.
59 Salvarani C, Gabriel SE, Gertz MA, Bjornsson J, Li C-Y, Hunder GG.
Primary systemic amyloidosis presenting as giant cell arteritis and
polymyalgia rheumatica. Arthritis Rheum 1994; 37: 162126.
60 Aiello PD, Trautmann JC, McPhee TJ, Kunselman AR, Hunder GG.
Visual prognosis in giant cell arteritis. Ophthalmology 1993;
100: 55056.
61 Gonzalez-Gay MA, GarciaPorrua C, Llorca J, et al. Visual
manifestations of giant cell arteritis: trends and clinical spectrum in
161 patients. Medicine (Baltimore) 2000; 79: 28392.
62 Salvarani C, Hunder GG. Musculoskeletal manifestations in a
population-based cohort of patients with giant cell arteritis.
Arthritis Rheum 1999; 42: 125966.
63 Cantini F, Salvarani C, Olivieri I, et al. Remitting seronegative
symmetrical synovitis with pitting oedema (RS3PE) syndrome: a
prospective follow-up and magnetic resonance imaging study.
Ann Rheum Dis 1999; 58: 23036.
64 Gonzalez-Gay MA, Garcia-Porrua C, Amor-Dorado JC, Lorca J.
Giant cell arteritis without clinically evident vascular involvement in
a dened population. Arthritis Rheum 2004; 51: 27477.
65 Hayreh SS, Podhajsky PA, Zimmerman B. Occult giant cell
arteritis: ocular manifestations. Am J Ophthalmol 1998; 125: 52126.
66 Bongartz T and Matteson EL. Large-vessel involvement in giant cell
arteritis. Curr Opin Rheumatol 2006; 18: 1017.
67 Gonzalez-Gay MA, Garcia-Porrua C, Pineiro A, Pego-Reigosa R,
Llorca J, Hunder GG. Aortic aneurysm and dissection in patients
with biopsy-proven giant cell arteritis from northwestern Spain: a
population-based study. Medicine (Baltimore) 2004; 83: 33541.
68 Le Hello C, Lvesque H, Jeanton M, et al. Lower limb giant cell
arteritis and temporal arteritis : followup of 8 cases. J Rheumatol
2001; 28: 140712.
69 Caselli R, Hunder GG, Whisnant JP. Neurologic disease in
biopsy-proven giant cell (temporal) arteritis. Neurology 1988;
38: 35259.
70 Caselli R, Daube JR, Hunder GG, Whisnant JP. Peripheral
neuropathic syndromes in giant cell (temporal) arteritis. Neurology
1988; 38: 68589.
71 Gonzalez-Gay MA, Blanco R, Rodriguez-Valverde V, et al.
Permanent visual loss and cerebrovascular accidents in giant cell
arteritis: predictors and response to treatment. Arthritis Rheum
1998; 41: 1497504.
72 Larson TS, Hall S, Hepper NG, Hunder GG. Respiratory tract
symptoms as a clue to giant cell arteritis. Ann Intern Med 1984;
101: 59497.
73 Valstar MH, Terpstra WF, de Jong RS. Pericardial and pleural
eusion in giant cell arteritis. Am J Med 2003; 114: 70809.
74 Lie JT, Failoni DD, Davis DC Jr. Temporal arteritis with giant cell
aortitis, coronary arteritis, and myocardial infarction.
Arch Pathol Lab Med 1986; 110: 85760.
75 Bajocchi G, Zamorani G, Cavazza A, et al. Giant-cell arteritis of the
female genital tract associated with occult arteritis and FDG-PET
evidence of large vessel vasculitis. Clin Exp Rheumatol 2007;
25 (suppl 44): S3639.
76 Kariv R, Sidi Y, Gur H. Systemic vasculitis presenting as a
tumorlike lesion. Four case reports and an analysis of 79 reported
cases. Medicine (Baltimore) 2000; 79: 34959.
Seminar
244 www.thelancet.com Vol 372 July 19, 2008
77 Luzar MJ, Whisler RL, Hunder GG. Syndrome of inappropriate
secretion of antidiruetic hormone in association with temporal
arteritis. J Rheumatol 1982; 9: 95760.
78 Lee CC, Su WW, Hunder GG. Dysarthria associated with giant cell
arteritis. J Rheumatol 1999; 26: 93132.
79 Cantini F, Salvarani C, Olivieri I, et al. Erythrocyte sedimentation
rate and C-reactive protein in the evaluation of disease activity and
severity in polymyalgia rheumatica: a prospective follow-up study.
Semin Arthritis Rheum 2000; 30: 1724.
80 Salvarani C, Hunder GG. Giant cell arteritis with low erythrocyte
sedimentation rate: frequency of occurrence in a population-based
study. Arthritis Rheum 2001; 45: 14045.
81 Hayreh SS, Podhajsky PA, Raman R, Zimmerman B. Giant cell
arteritis: validity and reliability of various diagnostic criteria.
Am J Ophthalmol 1997; 123: 28596.
82 Weyand CM, Fulbright JW, Evans JM, Hunder GG, Goronzy JJ.
Corticosteroid requirements in polymyalgia rheumatica.
Arch Intern Med 1999; 159: 57784.
83 Salvarani C, Cantini F, Niccoli L, et al. Acute phase response
reactants and the risk of developing relapse/recurrence in
polymyalgia rheumatica: a prospective follow up study.
Arthritis Rheum 2005; 53: 3338.
84 Lopez-Hoyos M, Ruiz de Alegria C, Blanco R, et al. Clinical utility
of anti-CCP antibodies in the dierential diagnosis of elderly-onset
rheumatoid arthritis and polymyalgia rheumatica. Rheumatology
2004; 43: 65557.
85 Gonzalez-Gay MA, Lopez-Diaz MJ, Barros S, et al. Giant cell
arteritis: laboratory tests at the time of diagnosis in a series of
240 patients. Medicine (Baltimore) 2005; 84: 27790.
86 ODuy JD, Wahner HW, Hunder GG. Joint imaging in
polymyalgia rheumatica. Mayo Clin Proc 1976; 51: 51924.
87 Salvarani C, Cantini F, Olivieri I, et al. Proximal bursitis in active
polymyalgia rheumatica. Ann Intern Med 1997; 27: 2731.
88 Cantini F, Salvarani C, Olivieri I, et al. Shoulder ultrasonography in
the diagnosis of polymyalgia rheumatica: a case-control study.
J Rheumatol 2001; 28: 104955.
89 Cantini F, Niccoli L, Nannini C, et al. Inammatory changes of hip
synovial structures in polymyalgia reumatica. Clin Exp Rheumatol
2005; 23: 46268.
90 Cantini F, Salvarani C, Olivieri I, et al. Inamed shoulder structures
in polymyalgia rheumatica with normal erythrocyte sedimentation
rate. Arthritis Rheum 2001; 44: 115559.
91 Salvarani C, Silingardi M, Ghirarduzzi A, et al. Is duplex
ultrasonography useful for the diagnosis of giant cell arteritis?
Ann Intern Med 2002; 137: 23238.
92 Karassa FB, Matsagas MI, Schmidt WA, Ioannidis JPA.
Meta-analysis: test performance of ultrasonography for giant cell
arteritis. Ann Intern Med 2005; 142: 35969.
93 Bley TA, Weiben O, Uhl M, et al. Assessment of the cranial
involvement pattern of giant cell arteritis with 3T magnetic
resonance imaging. Arthritis Rheum 2005; 52: 247077.
94 Stanson AW. Imaging ndings in extracranial (giant cell)
temporal arteritis. Clin Exp Rheumatol 2001;
18 (suppl 20): S4348.
95 Schmidt WA, Natusch A, Mller DE, Vorpahl K,
Gromnica-Ihle E. Involvement of peripheral arteries in giant cell
arteritis: a color Doppler sonography study. Clin Exp Rheumatol
2002; 20: 30918.
96 Blockmans D, de Ceuninck L, Vanderschueren S, Knockaert D,
Mortelmans L, Bobbaers H. Repetitive 18F-uorodeoxyglucose
positron emission tomography in giant cell arteritis: a prospective
study of 35 patients. Arthritis Rheum 2006; 55: 13137.
97 Gonzalez-Gay MA, Garcia-Porrua C, Salvarani C, Olivieri I,
Hunder GG. The spectrum of conditions mimicking polymyalgia
rheumatica in Northwestern Spain. J Rheumatol 2000;
27: 217984.
98 McCarty DJ, ODuy JD, Pearson L, Hunter JB. Remitting
seronegative symmetrical synovitis with pitting edema. RS3PE
syndrome. JAMA 1985; 254: 276367.
99 Olivieri I, Salvarani C, Cantini F. Remitting distal extremity swelling
with pitting edema: a distinct syndrome or a clinical feature of
dierent inammatory rheumatic diseases? J Rheumatol 1997;
24: 24952.
100 Olivieri I, Garcia-Porrua C, Padula A, Cantini F, Salvarani C,
Gonzalez-Gay MA. Late onset spondyloarthritis presenting with
polymyalgia rheumatica features: description of 7 cases.
Rheumatology Int 2007; 27: 92733.
101 Pego-Reigosa JM, Rodriguez-Rodriguez M, Hurtado-Hernandez Z,
et al. Calcium pyrophosphate deposition disease mimicking
polymyalgia rheumatica: a prospective followup study of predictive
factors for this condition in patients presenting with polymyalgia
symptoms. Arthritis Rheum 2005; 53: 93138.
102 Hopkinson ND, Shawe DJ, Gumpel JM. Polymyositis, not
polymyalgia rheumatica. Ann Rheum Dis 1991; 50: 32122.
103 Niccoli L, Salvarani C, Baroncelli G, Padula A, Olivieri I, Cantini F.
Renal cell carcinoma mimicking polymyalgia rheumatica. Clues for
a correct diagnosis. Scand J Rheumatol 2002; 31: 10306.
104 Churcill MA, Geraci HJE, Hunder GG. Musculoskeletal
manifestations of bacterial endocarditis. Ann Intern Med 1977;
87: 75459.
105 Pipitone N, Salvarani C. Are steroids alone sucient for the
treatment of giant cell arteritis? Best Pract Res Clin Rheumatol 2005;
19: 27792.
106 Hayreh SS, Zimmerman B, Kardon RH: Visual improvement with
corticosteroid therapy in giant cell arteritis. Report of a large study
and review of literature. Acta Ophthalmol Scand 2002; 80: 35567.
107 Mazlumzadeh M, Hunder GG, Easley KA, et al. Treatment of giant
cell arteritis using induction therapy with high-dose glucocorticoids:
a double-blind, placebo-controlled, randomized prospective clinical
trial. Arthritis Rheum 2006; 54: 331018.
108 Chevalet P, Barrier JH, Pottier P, et al. A randomized, multicenter,
controlled trial using intravenous pulses of mrthylprednisolone in
the initial treatment of simple forms of giant cell arteritis: a one
year followup study of 164 patients. J Rheumatol 2000; 27: 148491.
109 Hunder GG, Sheps SG, Allen GL, Joyce JW. Daily and alternate-day
corticosteroid regimens in treatment of giant cell arteritis:
comparison in a prospective study. Ann Intern Med 1975; 82: 61318.
110 Andersson R, Malmvall B-E, Bengtsson B-A. Long-term
corticosteroid treatment in giant cell arteritis. Acta Med Scand 1986;
220: 46569.
111 Proven A, Gabriel SE, Orces C, OFallon WM, Hunder GG.
Glucocorticoid therapy in giant cell arterits: duration and adverse
outcomes. Arthritis Rheum 2003; 49: 70308.
112 Jover JA, Hernandez-Garcia C, Morado IC, Vargas E, Banares A,
Fernandez-Gutierrez B. Combined treatment of giant-cell arteritis
with methotrexate and prednisone: a randomized, double-blind,
placebo-controlled trial. Ann Intern Med 2001; 134: 10614.
113 Homan GS, Cid MC, Hellmann DB, et al. A multicenter,
randomized, double-blind, placebo-controlled trial of adjuvant
methotrexate treatment for giant cell arteritis. Arthritis Rheum 2002;
46: 130918.
114 Weyand CM, Fulbright JW, Hunder GG, Evans JM, Goronzy JJ.
Treatment of giant cell arteritis: interleukin-6 as a biologic marker
of disease activity. Arthritis Rheum 2000; 43: 104148.
115 Recommendations for the prevention and treatment of
glucocorticoid-induced osteoporosis: 2001 update. American
College of Rheumatology Ad Hoc Committee on
Glucocorticoid-Induced Osteoporosis. Arthritis Rheum 2001;
44: 1496503.
116 Sambrook PN. How to prevent steroid induced osteoporosis.
Ann Rheum Dis 2005; 64: 17678
117 Spiera RF, Mitnick HJ, Kupersmith M, et al. A prospective,
double-blind, randomized, placebo controlled trial of methotrexate
in the treatment of giant cell arteritis (GCA). Clin Exp Rheumatol
2001; 19: 495501.
118 Mahr AD, Jover JA, Spiera RF, Hernandez-Garcia C,
Fernandez-Gutierrez B, LaValley MP, Merkel PA. Adjunctive
methotrexate for treatment of giant cell arteritis. An individual
patient data meta-analysis. Arthritis Rheum 2007; 56: 278997.
119 De Silva M, Hazleman BL. Azathioprine in giant cell
arteritis/polymyalgia rheumatica: a double-blind study.
Ann Rheum Dis 1986; 45: 13638.
120 Homan GS, Cid MC, Rendt-Zagar KE, et al. Iniximab for
maintenance of glucocorticosteroid-induced remission of giant
cell arteritis: a randomized trial. Ann Intern Med 2007;
146: 62130.
Seminar
www.thelancet.com Vol 372 July 19, 2008 245
121 Hernandez-Rodriguez J, Segarra M, Vilardell C, et al. Tissue
production of pro-inammatory cytokines (IL-1beta, TNFalpha and
IL-6) correlates with the intensity of the systemic inammatory
response and with corticosteroid requirements in giant-cell arteritis.
Rheumatology (Oxford) 2004; 43: 294301.
122 Cantini F, Niccoli L, Salvarani C, Padula A, Olivieri I. Treatment of
longstanding active giant cell arteritis with iniximab: report of four
cases. Arthritis Rheum 2001; 44: 293335.
123 Nesher G, Berkun Y, Mates M, Baras M, Rubinow A,
Sonnenblick M. Low-dose aspirin and prevention of cranial
ischemic complications in giant cell arteritis. Arthritis Rheum 2004;
50: 133237.
124 Lee MS, Smith SD, Galor A, Homan GS. Antiplatelet and
anticoagulant therapy in patients with giant cell arteritis.
Arthritis Rheum 2006; 54: 330609.
125 Weyand CM, Kaiser M, Yang H, Younge B, Goronzy JJ. Therapeutic
eects of acetysalcylic acid in giant cell arteritis. Arthritis Rheum
2002; 46: 45766.
126 Salvarani C, Cantini F, Boiardi L, Hunder GG. Polymyalgia
rheumatica. Best Pract Res Clin Rheumatol 2004; 18: 70522.
127 Kremers HM, Reinalda MS, Crowson CS, Zinsmeister AR,
Hunder GG, Gabriel SE. Relapse in a population based cohort of
patients with polymyalgia rheumatica. J Rheumatol 2005; 32: 6573.
128 Ayoub WT, Franklin CM, Torretti D. Polymyalgia rheumatica:
duration of therapy and long-term outcome. Am J Med 1985;
79: 30915.
129 Gabriel SE, Sunku J, Salvarani C, OFallon WM, Hunder GG.
Adverse outcomes of anti-inammatory therapy among patients
with polymyalgia rheumatica. Arthritis Rheum 1997; 40: 187378.
130 Caporali R, Cimmino MA, Ferraccioli G, et al. Prednisone plus
methotrexate for polymyalgia rheumatica: a randomized,
double-blind, placebo-controlled trial. Ann Intern Med 2004;
141: 493500.
131 Salvarani C, Cantini F, Niccoli L, et al. Treatment of refractory
polymyalgia rheumatica with iniximab: a pilot study. J Rheumatol
2003; 30: 76063.
132 Catanoso MG, Macchioni PL, Boiardi L, Pipitone N, Salvarani C.
Treatment of refractory polymyalgia rheumatica with etanercept:
an open pilot study. Arthritis Rheum 2007; 57: 151419.
133 Salvarani C, Macchioni PL, Manzini C, et al. Iniximab plus
prednisone or placebo plus prednisone for the initial treatment of
polymyalgia rheumatica. A randomized trial. Ann Intern Med 2007;
146: 63139.
134 Strand V, Yazici Y. Interleukin-6 inhibition. Tolerability prole and
clinical implications. Bull NYU Hosp JT Dis 2007; 65 (suppl 1): S2124.
135 Davis PM, Nadler SG, Stetsko DK, Suchard SJ. Abatacept modulates
human dendritic cell-stimulated T-cell proliferation and eector
function independent of IDO induction. Clin Immunol 2008;
126: 3847.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Neurointervensi PDFDocument525 pagesNeurointervensi PDFAsri Kartika Anggraeni100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Chelox Therapy For HeartDocument4 pagesChelox Therapy For HeartrounakshahNo ratings yet
- 2018 043 00060 FU3 - Investigator Safety Alert Letter - 1541503583 PDFDocument14 pages2018 043 00060 FU3 - Investigator Safety Alert Letter - 1541503583 PDFComan IoanaNo ratings yet
- BSN3A Summative Test (Prelim)Document16 pagesBSN3A Summative Test (Prelim)Emuelle GanNo ratings yet
- Cath Lab - Interventional Radiology Nursing Skills ChecklistDocument7 pagesCath Lab - Interventional Radiology Nursing Skills Checklistdk15janNo ratings yet
- Application Training enDocument96 pagesApplication Training enscuby660No ratings yet
- The JKL Medical DictionaryDocument186 pagesThe JKL Medical Dictionarymoekyaw7171No ratings yet
- ESC Guidelines On The Diagnosis and Treatment of Peripheral Artery DiseasesDocument56 pagesESC Guidelines On The Diagnosis and Treatment of Peripheral Artery DiseasesJuan José Ruiz CastilloNo ratings yet
- Manual Servicio bv29Document123 pagesManual Servicio bv29newplayer12100% (1)
- QuickCat BrochureDocument3 pagesQuickCat Brochurebiomedical_com_brNo ratings yet
- Seminar: Jan Claassen, Soojin ParkDocument17 pagesSeminar: Jan Claassen, Soojin ParkRaul DoctoNo ratings yet
- Hemorrhagic Unilateral RetinopathyDocument7 pagesHemorrhagic Unilateral RetinopathyHanna_RNo ratings yet
- AortographyDocument31 pagesAortographyWendy Escalante100% (1)
- AngiographyDocument17 pagesAngiographyPimsiree MameawNo ratings yet
- Craniocervical Arterial VariationsDocument171 pagesCraniocervical Arterial VariationsMircea JunbeiNo ratings yet
- Full Download Test Bank For Introduction To Radiologic and Imaging Sciences and Patient Care 7th Edition by Adler PDF Full ChapterDocument35 pagesFull Download Test Bank For Introduction To Radiologic and Imaging Sciences and Patient Care 7th Edition by Adler PDF Full Chapternarwhalunaware4zjh6d100% (18)
- Edexcel GCE: Biology (Salters-Nuffield)Document20 pagesEdexcel GCE: Biology (Salters-Nuffield)samira_666No ratings yet
- Cervical VertigoDocument42 pagesCervical VertigoIka Ayu ParamitaNo ratings yet
- CTO GuideDocument14 pagesCTO GuideTeodor BicaNo ratings yet
- Icare EIDON Family REV002 Hi ResDocument7 pagesIcare EIDON Family REV002 Hi ResPramod UpadhyayNo ratings yet
- ATLAS OCT-A-IN AMD EbookDocument152 pagesATLAS OCT-A-IN AMD EbookMAJO100% (2)
- AngografiDocument6 pagesAngografiMulyadiNo ratings yet
- SOMATOM Definition Flash: Answers For LifeDocument48 pagesSOMATOM Definition Flash: Answers For LifepeymanNo ratings yet
- Assumption EDocument6 pagesAssumption EValentyn KhmarskyiNo ratings yet
- 1 s2.0 S1930043321003083 MainDocument5 pages1 s2.0 S1930043321003083 MainSandra ArellanoNo ratings yet
- ICD9CM-Procedure Index-A5Document274 pagesICD9CM-Procedure Index-A5Rosdiana OceNo ratings yet
- ISICAM TimetableDocument8 pagesISICAM TimetableMichael SusantoNo ratings yet
- Onyx IFUDocument48 pagesOnyx IFUMamdooh AlqathamiNo ratings yet
- Childhood Vasculitis: Sujata SawhneyDocument9 pagesChildhood Vasculitis: Sujata SawhneyErick HernandezNo ratings yet
- Multi-Slice CT For Coronary Calcium Scoring and Coronary AngiographyDocument63 pagesMulti-Slice CT For Coronary Calcium Scoring and Coronary AngiographyAnnisaa FitrianiNo ratings yet