You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Oral Cancer Grading SystemDocument42 pagesOral Cancer Grading SystemMadhura ShekatkarNo ratings yet
- Sistema de ParisDocument177 pagesSistema de ParisNabor Gallo100% (1)
- Breast DisorderDocument89 pagesBreast DisorderYang TayengNo ratings yet
- Laboratory Diagnosis of Cancer Morphologic MethodsDocument7 pagesLaboratory Diagnosis of Cancer Morphologic MethodsRafaih KhanNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
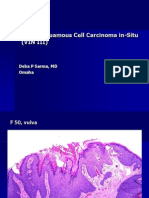
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
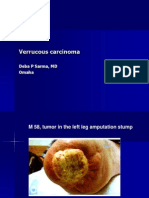
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
- Malignant Tumors of Oral LocalizationDocument49 pagesMalignant Tumors of Oral LocalizationMladen PazinNo ratings yet
- Anticancer Cow UrineDocument25 pagesAnticancer Cow UrineSameer AgrawalNo ratings yet
- Liceo de Cagayan University: General Pathology and Histo-Techniques (Laboratory)Document3 pagesLiceo de Cagayan University: General Pathology and Histo-Techniques (Laboratory)Rose Jaren Mae AbraganNo ratings yet
- 14 CR Muthia Ovarian Clear Cell Carcinoma Which Detected in Ascitic Fluid SmearDocument8 pages14 CR Muthia Ovarian Clear Cell Carcinoma Which Detected in Ascitic Fluid Smearmuttaqin95No ratings yet
- Bladder TumorDocument32 pagesBladder TumorAngelynChristabellaNo ratings yet
- Atlas de CitologíaDocument76 pagesAtlas de CitologíaSujeyCasimiroNo ratings yet
- Ovary, Fallopian Tube, Primary Peritoneal Carcinoma TNM, 8th Ed - UpToDateDocument3 pagesOvary, Fallopian Tube, Primary Peritoneal Carcinoma TNM, 8th Ed - UpToDateSol anonimoNo ratings yet
- Surgical Pathology - Major and Minor Salivary GlandsDocument2 pagesSurgical Pathology - Major and Minor Salivary GlandsIsabel CastilloNo ratings yet
- Critical Illness Policy WordingDocument10 pagesCritical Illness Policy WordingFigoNo ratings yet
- Makalah Bahasa Inggris NewDocument25 pagesMakalah Bahasa Inggris Newmei diana sara'isNo ratings yet
- NeoplasiaDocument9 pagesNeoplasiaRinaldo GintingNo ratings yet
- Third Eyelid Gland Neoplasms of Dogs and CatsDocument6 pagesThird Eyelid Gland Neoplasms of Dogs and CatsMicheleBerselliNo ratings yet
- 2.2.1 Part 2Document3 pages2.2.1 Part 2Michal BonarNo ratings yet
- Filesugd66484b .PDF 2Document75 pagesFilesugd66484b .PDF 2صاحب القلمNo ratings yet
- Common SLE Questions - OziDentDocument34 pagesCommon SLE Questions - OziDentnnawaz40% (1)
- Cellular AberrationDocument71 pagesCellular AberrationMichael CoronadoNo ratings yet
- Anal Cancer IndiaDocument14 pagesAnal Cancer Indiaindia_wecareNo ratings yet
- Breast CarcinomasDocument19 pagesBreast CarcinomasGirkati ShivaniNo ratings yet
- Group C Report FinalDocument57 pagesGroup C Report FinalRI NANo ratings yet
- Sinonasal Undifferentiated Carcinoma (SNUC)Document13 pagesSinonasal Undifferentiated Carcinoma (SNUC)Anonymous VTZ0bL5Od7No ratings yet
- Life Secure Brochure - 1Document13 pagesLife Secure Brochure - 1spikysanchitNo ratings yet
- Neoplasia: Dr. Phoo Pwint Maw KhineDocument28 pagesNeoplasia: Dr. Phoo Pwint Maw KhineThinagari JevataranNo ratings yet
- Ijphrd Journal July-Sep 2013 - 06-06-213 PDFDocument307 pagesIjphrd Journal July-Sep 2013 - 06-06-213 PDFp1843dNo ratings yet
- NCM 41118L Final Quiz 3Document13 pagesNCM 41118L Final Quiz 3Matelyn OargaNo ratings yet
- IRDAI - Optional Items Excluded - July 2016Document92 pagesIRDAI - Optional Items Excluded - July 2016Jerome GelfandNo ratings yet
- Case Ca Laring UMJDocument51 pagesCase Ca Laring UMJDera Seta SaputriNo ratings yet