You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ship Building and RepairingDocument37 pagesShip Building and RepairingOsama Awad100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- APDocument7 pagesAPRaviKiran AvulaNo ratings yet
- Sampling and Sample SurveyDocument15 pagesSampling and Sample SurveySUFIAUN FERDOUS100% (1)
- BTS - Volume I Main Report PDFDocument214 pagesBTS - Volume I Main Report PDFAlbert Mwauzi100% (1)
- Chronic Pain Management Fact SheetDocument2 pagesChronic Pain Management Fact SheetAdvaMedLCINo ratings yet
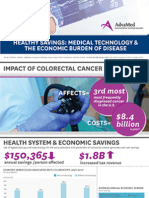
- Infographic: IMPACT OF COLORECTAL CANCERDocument1 pageInfographic: IMPACT OF COLORECTAL CANCERAdvaMedLCINo ratings yet
- Infographic: IMPACT OF HEART DISEASEDocument1 pageInfographic: IMPACT OF HEART DISEASEAdvaMedLCINo ratings yet
- 2015 Innovation AgendaDocument1 page2015 Innovation AgendaAdvaMedLCINo ratings yet
- Innovation Agenda: February 2015Document4 pagesInnovation Agenda: February 2015AdvaMedLCINo ratings yet
- The Anatomy of Medical ResearchDocument16 pagesThe Anatomy of Medical ResearchAdvaMedLCI0% (1)
- Pulse Redefining Medical Technology InnovationDocument64 pagesPulse Redefining Medical Technology InnovationAdvaMedLCINo ratings yet
- Innovation Scorecard - Report FINAL - External UNSECUREDDocument50 pagesInnovation Scorecard - Report FINAL - External UNSECUREDAdvaMedLCINo ratings yet
- Oct 2012 King Report FINALDocument16 pagesOct 2012 King Report FINALAdvaMedLCINo ratings yet
- Primary Secondary SourcesDocument17 pagesPrimary Secondary SourcesBrandee Davis BergumNo ratings yet
- C D R No. o F Deaths A Year Total Mid Year Population: Demography and Urbanisation NotesDocument49 pagesC D R No. o F Deaths A Year Total Mid Year Population: Demography and Urbanisation NotesSanjay KumarNo ratings yet
- 1 ListDocument16 pages1 ListSanjay KoriNo ratings yet
- BDM 1Document34 pagesBDM 1Ajay Kumar SharmaNo ratings yet
- Census 2011 Lakhisarai PDFDocument548 pagesCensus 2011 Lakhisarai PDFvikas.k.netNo ratings yet
- 2015 CPH - Report No. 2 - PhilippinesDocument248 pages2015 CPH - Report No. 2 - PhilippinesCasey Maureen ArrezaNo ratings yet
- Summary and Statistical Report of The 2007Document113 pagesSummary and Statistical Report of The 2007ekaitzbengoetxea85789% (19)
- Pakistan Bureau of StatisticsDocument7 pagesPakistan Bureau of Statisticsarizwan123No ratings yet
- Question 818403Document5 pagesQuestion 818403rajdeep JaiswalNo ratings yet
- Occ MindoroDocument269 pagesOcc MindoroElleason Joshua G. FranciscoNo ratings yet
- 9 A Vision IAS Prelims 2020 TestDocument43 pages9 A Vision IAS Prelims 2020 TestGaurav MeenaNo ratings yet
- Census of India 1961: MadrasDocument72 pagesCensus of India 1961: Madrasanusha shinyNo ratings yet
- TanzaniaDocument10 pagesTanzaniahst939No ratings yet
- Bakare Aishat Damilola Project Computer Science Design and Implementation of ComputerDocument52 pagesBakare Aishat Damilola Project Computer Science Design and Implementation of ComputerMICHAEL ADEYEMONo ratings yet
- Consumer and Industrial Buying Behaviour: Assignment No. 1Document9 pagesConsumer and Industrial Buying Behaviour: Assignment No. 1Manu MnNo ratings yet
- Introduction To Statistics: Prepared By: Engr. Gilbey'S Jhon - Ladion InstructorDocument25 pagesIntroduction To Statistics: Prepared By: Engr. Gilbey'S Jhon - Ladion InstructorMark B. BarrogaNo ratings yet
- Human Rights Commission - Shaista Shameem - OpinionDocument32 pagesHuman Rights Commission - Shaista Shameem - OpinionIntelligentsiya HqNo ratings yet
- District Census Handbook JaipurDocument578 pagesDistrict Census Handbook JaipurAnshu BhargavaNo ratings yet
- Chamrajnagar Census 2001 PDFDocument384 pagesChamrajnagar Census 2001 PDFManjunath JadhavNo ratings yet
- 2018042016Document186 pages2018042016SanjeetNo ratings yet
- Open Doors: Extending Hospitality To Travelers With DisabilitiesDocument37 pagesOpen Doors: Extending Hospitality To Travelers With DisabilitiesAda MaudeNo ratings yet
- Demographic For HealthDocument77 pagesDemographic For HealthDahir100% (1)
- Labor Migration Statistics in ASEANDocument128 pagesLabor Migration Statistics in ASEANjvtignoNo ratings yet
- DH 2011 0904 Part A DCHB MoradabadDocument578 pagesDH 2011 0904 Part A DCHB MoradabadInnovian SolutionsNo ratings yet
- The Potential For Growing Marine Leisure PDFDocument160 pagesThe Potential For Growing Marine Leisure PDFcottardNo ratings yet
- UPU Addressing Conference: Including S42 Recognition CeremonyDocument4 pagesUPU Addressing Conference: Including S42 Recognition CeremonycbetterNo ratings yet