You might also like
- Tietz's Applied Laboratory MedicineFrom EverandTietz's Applied Laboratory MedicineMitchell G. ScottRating: 3 out of 5 stars3/5 (1)
- Handbook of Histopathological and Histochemical Techniques: Including Museum TechniquesFrom EverandHandbook of Histopathological and Histochemical Techniques: Including Museum TechniquesRating: 4.5 out of 5 stars4.5/5 (13)
- Agglutination, Complement, Neutralization, and Inhibition: Methods in Immunology and Immunochemistry, Vol. 4From EverandAgglutination, Complement, Neutralization, and Inhibition: Methods in Immunology and Immunochemistry, Vol. 4No ratings yet
- Senior Medical Laboratory Technician: Passbooks Study GuideFrom EverandSenior Medical Laboratory Technician: Passbooks Study GuideNo ratings yet
- Practical Manual for Detection of Parasites in Feces, Blood and Urine SamplesFrom EverandPractical Manual for Detection of Parasites in Feces, Blood and Urine SamplesNo ratings yet
- The Diverse Faces of Bacillus CereusFrom EverandThe Diverse Faces of Bacillus CereusVincenzo SaviniNo ratings yet
- Clinical Biochemistry: Contemporary Theories and TechniquesFrom EverandClinical Biochemistry: Contemporary Theories and TechniquesHerbert SpiegelNo ratings yet
- Biotechnology: A Laboratory CourseFrom EverandBiotechnology: A Laboratory CourseRating: 5 out of 5 stars5/5 (1)
- Microbiological Guidelines: Support for Interpretation of Microbiological Test Results of FoodsFrom EverandMicrobiological Guidelines: Support for Interpretation of Microbiological Test Results of FoodsNo ratings yet
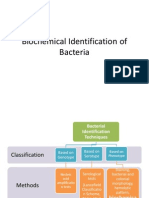
- Biochemical Identification of BacteriaDocument72 pagesBiochemical Identification of BacteriaMaria Jhoyce MagpantayNo ratings yet
- Manual of Antimicrobial Susceptibility TestingDocument241 pagesManual of Antimicrobial Susceptibility TestingEndale Balcha100% (4)
- StainingDocument60 pagesStainingved.g007No ratings yet
- Medical TechnologyDocument13 pagesMedical Technologyangelina buenaNo ratings yet
- AgglutinationDocument15 pagesAgglutinationmma1976No ratings yet
- Minimal Inhibitory Concentration TestDocument26 pagesMinimal Inhibitory Concentration TestZandhika Alfi PratamaNo ratings yet
- Discuss The Various Theories On The Gram Stain.: Gram-Negative Bacteria Gram-Positive BacteriaDocument5 pagesDiscuss The Various Theories On The Gram Stain.: Gram-Negative Bacteria Gram-Positive BacteriaFiddo Waggay100% (3)
- Culture Media & Culture MethodsDocument25 pagesCulture Media & Culture Methodsryan100% (1)
- Microbiology PDFDocument71 pagesMicrobiology PDFDanny Alexander TullumeNo ratings yet
- MLT Blood Bank Exam 2 FullDocument4 pagesMLT Blood Bank Exam 2 Fullkasdf gre bbtNo ratings yet
- Antibiotic ResistanceDocument32 pagesAntibiotic ResistanceEmine Alaaddinoglu100% (2)
- Sterilization and DisinfectionDocument10 pagesSterilization and DisinfectiondrugdrugNo ratings yet
- District Laboratory Practice in Tropical Countries, Color PlatesDocument20 pagesDistrict Laboratory Practice in Tropical Countries, Color Platesسجدةللرحمان100% (1)
- Microbial Culture MediaDocument9 pagesMicrobial Culture Mediaማላያላም ማላያላም100% (2)
- Ciulla - MycoDocument13 pagesCiulla - MycoSalve Rachelle BillenaNo ratings yet
- Antigen Presenting CellsDocument27 pagesAntigen Presenting CellsSajjad AhmadNo ratings yet
- ANTIMICROBIAL ResistanceDocument4 pagesANTIMICROBIAL ResistancePuspa Das100% (1)
- Biosafety Measures in Microbiology LabsDocument56 pagesBiosafety Measures in Microbiology LabsPramod50% (2)
- Special StainsDocument15 pagesSpecial StainsEl Marie SalungaNo ratings yet
- BacteriologyDocument75 pagesBacteriologyHoward BarlomentoNo ratings yet
- Basic Immunology 2014 9Document35 pagesBasic Immunology 2014 9nazargafarNo ratings yet
- MLT Blood Bank Exam 4 FullDocument3 pagesMLT Blood Bank Exam 4 Fullkasdf gre bbtNo ratings yet
- SerologyDocument442 pagesSerologyPura Javier100% (2)
- BIOL 142 General Microbiology Lab ManualDocument91 pagesBIOL 142 General Microbiology Lab Manualasad bashirNo ratings yet
- Compre-ASCP-Parts 2 and 3 PDFDocument20 pagesCompre-ASCP-Parts 2 and 3 PDFCyp Gabriel Esteba Peñaflorida100% (1)
- Clinical Lab DilutionsDocument19 pagesClinical Lab DilutionsAlex Joshua Maglasang100% (1)
- Introduction to Mycology: An Overview of Fungal Morphology and ReproductionDocument26 pagesIntroduction to Mycology: An Overview of Fungal Morphology and ReproductionOsannah Irish InsongNo ratings yet
- Gram Staining Reveals Pink BacteriaDocument9 pagesGram Staining Reveals Pink BacteriaKristine Boholst100% (1)
- Enterobius Vermicularis: Ciulla Chapter 8 - ParasitologyDocument13 pagesEnterobius Vermicularis: Ciulla Chapter 8 - ParasitologySalve Rachelle BillenaNo ratings yet
- Microbio Lab 6Document4 pagesMicrobio Lab 6api-374321750% (2)
- Antimicrobial Susceptibility Testing - Primer For CliniciansDocument20 pagesAntimicrobial Susceptibility Testing - Primer For Cliniciansdipzhit100% (1)
- Mycology Lab2Document7 pagesMycology Lab2api-3700579100% (1)
- Culture Media and MethodsDocument100 pagesCulture Media and MethodsAnsh Dutta100% (1)
- Introduction To Histology and Histological TechniquesDocument42 pagesIntroduction To Histology and Histological TechniquesGeoffreyNo ratings yet
- Microbiology Exam 23408Document5 pagesMicrobiology Exam 23408juliasun888350% (2)
- Antimicrobial Susceptibility Testing PDFDocument19 pagesAntimicrobial Susceptibility Testing PDFdatitoxNo ratings yet
- Mycology Lab3Document2 pagesMycology Lab3api-370057950% (2)
- Review Question For Comprehensive Exam in BBDocument6 pagesReview Question For Comprehensive Exam in BBEllen Castillo MarianoNo ratings yet
- Candida Urinary Tract Infections-TreatmentDocument10 pagesCandida Urinary Tract Infections-TreatmentsummiyaNo ratings yet
- Candida UTI DiagnosisDocument5 pagesCandida UTI DiagnosissummiyaNo ratings yet
- Update 2014, 7 Discontinuation of Salmonella Serology Test AKUHDocument1 pageUpdate 2014, 7 Discontinuation of Salmonella Serology Test AKUHsummiyaNo ratings yet
- Critically Ill Elderly Man with Disseminated Candidiasis Following Colonic SurgeryDocument20 pagesCritically Ill Elderly Man with Disseminated Candidiasis Following Colonic SurgerysummiyaNo ratings yet
- Candidiasis MedscapeDocument36 pagesCandidiasis MedscapesummiyaNo ratings yet
- C-Reactive Protein (CRP) : Mohammad Zeeshan Resident MicrobiologyDocument30 pagesC-Reactive Protein (CRP) : Mohammad Zeeshan Resident MicrobiologysummiyaNo ratings yet
- Candidemia in Neonatal ICU - Experience From A Tertiary Care HospitalDocument5 pagesCandidemia in Neonatal ICU - Experience From A Tertiary Care HospitalsummiyaNo ratings yet
- Candida UTI TreatmentDocument10 pagesCandida UTI TreatmentsummiyaNo ratings yet
- Candidemia in Neonatal ICU - Experience From A Tertiary Care HospitalDocument5 pagesCandidemia in Neonatal ICU - Experience From A Tertiary Care HospitalsummiyaNo ratings yet
- Trypanosoma MCQDocument2 pagesTrypanosoma MCQsummiya100% (2)
- Dengue Infection in Cancer Patients: Department of MedicineDocument18 pagesDengue Infection in Cancer Patients: Department of MedicinesummiyaNo ratings yet
- Vaccine Updates UkDocument4 pagesVaccine Updates UksummiyaNo ratings yet
- Diabetes Patient Develops Mucormycosis After ChemotherapyDocument32 pagesDiabetes Patient Develops Mucormycosis After ChemotherapysummiyaNo ratings yet
- Cases in TransplantationDocument59 pagesCases in TransplantationsummiyaNo ratings yet
- Id SuggestionDocument2 pagesId SuggestionsummiyaNo ratings yet
- Case 8 TBDocument41 pagesCase 8 TBsummiyaNo ratings yet
- Bio SafetyDocument68 pagesBio SafetysummiyaNo ratings yet
- CASE FILES Hiv MeaslesDocument15 pagesCASE FILES Hiv MeaslessummiyaNo ratings yet
- Congenital Hydrocephalus Child With VP Shunt Obstruction And Ceftriaxone Resistant E. coli CSF InfectionDocument15 pagesCongenital Hydrocephalus Child With VP Shunt Obstruction And Ceftriaxone Resistant E. coli CSF InfectionsummiyaNo ratings yet
- Bio SafetyDocument68 pagesBio SafetysummiyaNo ratings yet
- An Unusual Cause of Osteomyelitis: DR Summiya NizamuddinDocument43 pagesAn Unusual Cause of Osteomyelitis: DR Summiya NizamuddinsummiyaNo ratings yet
- Blood Culture Collection 2Document14 pagesBlood Culture Collection 2summiyaNo ratings yet
- Antigen-Antibody Interactions: Principles of ImmunologyDocument27 pagesAntigen-Antibody Interactions: Principles of ImmunologysummiyaNo ratings yet
- Bacterial ShapesDocument28 pagesBacterial ShapessummiyaNo ratings yet
- An Unusual Cause of Osteomyelitis: DR Summiya NizamuddinDocument43 pagesAn Unusual Cause of Osteomyelitis: DR Summiya NizamuddinsummiyaNo ratings yet
- 4-ZN StainDocument66 pages4-ZN StainsummiyaNo ratings yet
- Aspergillus and AspergillosisDocument35 pagesAspergillus and AspergillosissummiyaNo ratings yet
- Ag-Ab Reactions Tests For Ag-Ab ReactionsDocument36 pagesAg-Ab Reactions Tests For Ag-Ab ReactionssummiyaNo ratings yet
- Antigen-Antibody Interactions: Principles of ImmunologyDocument27 pagesAntigen-Antibody Interactions: Principles of ImmunologysummiyaNo ratings yet
- Elanco Parvovirus DXTX GDocument2 pagesElanco Parvovirus DXTX Gazamkhan60No ratings yet
- Spagyria vs Alchemy: Separating Myth from TruthDocument4 pagesSpagyria vs Alchemy: Separating Myth from Truthvas25No ratings yet
- 31.ergonomic Approach of Modification of Seat - EncDocument11 pages31.ergonomic Approach of Modification of Seat - EncSHASHANK ROHITNo ratings yet
- By hkdsegayau: 通識科 IES 滿分 Sample (樣本)Document10 pagesBy hkdsegayau: 通識科 IES 滿分 Sample (樣本)Chi Shing HoNo ratings yet
- Lean GuideDocument155 pagesLean GuideSujoy Kar100% (1)
- Diuretics MOA, Examples, Effects, and Nursing ConsiderationsDocument1 pageDiuretics MOA, Examples, Effects, and Nursing ConsiderationsGrace ButlerNo ratings yet
- Hyatt Amritsar showcases Chinese and Thai cuisineDocument1 pageHyatt Amritsar showcases Chinese and Thai cuisineAnmol MehanNo ratings yet
- GRADE 5 - WEEK 6 Catch UpDocument8 pagesGRADE 5 - WEEK 6 Catch Upbutchabdon1992No ratings yet
- Product Name: Clinical Chemistry Alkaline WashDocument11 pagesProduct Name: Clinical Chemistry Alkaline WashАндрей ФедуловNo ratings yet
- Kindergarten q1 Week10 v2Document33 pagesKindergarten q1 Week10 v2Aryan Angela Dela CruzNo ratings yet
- International Journal of Radiology and Imaging Technology Ijrit 7 082Document3 pagesInternational Journal of Radiology and Imaging Technology Ijrit 7 082Zafitri AsrulNo ratings yet
- Donald A. Neumann-Kinesiology of The Musculoskeletal SystemDocument607 pagesDonald A. Neumann-Kinesiology of The Musculoskeletal SystemLuciano Klapisch81% (16)
- Burnett: The First Non-Conformist HomeopathDocument4 pagesBurnett: The First Non-Conformist Homeopathsimiliadoc100% (1)
- Daftar PustakaDocument3 pagesDaftar PustakaErliTa TyarLieNo ratings yet
- 16 Potential Key Performance Indicators For HospitalsDocument3 pages16 Potential Key Performance Indicators For HospitalsSyed Murtuza BakshiNo ratings yet
- Mole Airlines, Emp. Form. ExcerciseDocument2 pagesMole Airlines, Emp. Form. ExcerciseKamariah IsmailNo ratings yet
- Cancer Fighting StrategiesDocument167 pagesCancer Fighting StrategiesCaptainjillNo ratings yet
- Slide PPT PrismaDocument31 pagesSlide PPT PrismaUlul Azmi AdnanNo ratings yet
- The Perspective of Vat Concessions Regime in Tanzania PDFDocument32 pagesThe Perspective of Vat Concessions Regime in Tanzania PDFHandley Mafwenga SimbaNo ratings yet
- Exercise Chart: Warm UpDocument1 pageExercise Chart: Warm UpJeremy van der MerweNo ratings yet
- Child Development A Cultural Approach 2nd Edition Arnett Solutions Manual DownloadDocument37 pagesChild Development A Cultural Approach 2nd Edition Arnett Solutions Manual DownloadMichael Pontius100% (24)
- Nursing Process in Drug TherapyDocument60 pagesNursing Process in Drug TherapyYra JhaneNo ratings yet
- Hospital Administrative Assistant Resume-A4Document2 pagesHospital Administrative Assistant Resume-A4Philip V AlexNo ratings yet
- Your Body Speaks Your Mind by Deb ShapiroDocument315 pagesYour Body Speaks Your Mind by Deb Shapiroisidora milosevic100% (2)
- 4th Quarter CAPSTONEDocument30 pages4th Quarter CAPSTONEWallace RamosNo ratings yet
- The ABO Blood Groups: Phenotypes GenotypesDocument2 pagesThe ABO Blood Groups: Phenotypes GenotypesSheila Mae CabahugNo ratings yet
- Veterans Handbook 2020Document69 pagesVeterans Handbook 2020Senator Cory BookerNo ratings yet
- Vulvovaginal Atrophy in The CRETA Study The Healthcare Professionals PerceptionDocument7 pagesVulvovaginal Atrophy in The CRETA Study The Healthcare Professionals PerceptionHugo GutiérrezNo ratings yet
- Health Promotion Prevention Plan Presentation (Capter 5)Document42 pagesHealth Promotion Prevention Plan Presentation (Capter 5)MuniraNo ratings yet
- Solutions For RefugeesDocument24 pagesSolutions For RefugeesjacquelineNo ratings yet