You might also like
- BacteriologyDocument36 pagesBacteriologyMuhammad Furqaan Bari100% (1)
- Pediatric Pulmonology 1Document156 pagesPediatric Pulmonology 1zaidaan100% (1)
- Jansen Koh SummaryDocument54 pagesJansen Koh SummaryLorraineYongNo ratings yet
- PARASITOLOGYDocument33 pagesPARASITOLOGYAli AhmedNo ratings yet
- Articles English TyphoidDocument13 pagesArticles English TyphoidSiDewiAjja100% (1)
- Sepsis 2013Document42 pagesSepsis 2013RatnaNo ratings yet
- Case Files® EnterococcusDocument4 pagesCase Files® EnterococcusAHMAD ADE SAPUTRANo ratings yet
- DM Lec 28-10Document46 pagesDM Lec 28-10s.zainabtanweerNo ratings yet
- C Ystic Fibrosis (CF) : Learning Issues For Tutorial 2 Cheryl Tompkins, Group 6Document3 pagesC Ystic Fibrosis (CF) : Learning Issues For Tutorial 2 Cheryl Tompkins, Group 6k2m1b6ksNo ratings yet
- Pyogenic Cocci Pyogenic Means " Pus Forming" Cocci Means "Spherical Bacteria"Document14 pagesPyogenic Cocci Pyogenic Means " Pus Forming" Cocci Means "Spherical Bacteria"Ab AbNo ratings yet
- Pseudomembranous Colitis Case ReportDocument18 pagesPseudomembranous Colitis Case ReportrizkyauliautamaNo ratings yet
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- L15 SalmonellaDocument19 pagesL15 SalmonellaMohammed RedhaNo ratings yet
- Epidemiology of Infectious Disease Amebiasis: University of Fallujah College of Medicine Community MedicineDocument7 pagesEpidemiology of Infectious Disease Amebiasis: University of Fallujah College of Medicine Community MedicineMohamed HamoodNo ratings yet
- Microbiology Last Moment RevisionDocument16 pagesMicrobiology Last Moment RevisionDeepak MainiNo ratings yet
- 伤寒英文教案 Typhoid Fever-应若素Document36 pages伤寒英文教案 Typhoid Fever-应若素Wai Kwong ChiuNo ratings yet
- Practical 4 Staphylococci PresentationDocument24 pagesPractical 4 Staphylococci PresentationPatrisha BuanNo ratings yet
- SGL 11Document29 pagesSGL 11fasdfNo ratings yet
- His To Plasm OsisDocument16 pagesHis To Plasm OsisDelyn Gamutan MillanNo ratings yet
- EnterobacteriaceaeDocument31 pagesEnterobacteriaceaeVivek ChaudharyNo ratings yet
- ShigellaDocument23 pagesShigellaAayush AdhikariNo ratings yet
- 9th Lec. Enterobacteriaceae Part 2 and Pseudo2023.Document30 pages9th Lec. Enterobacteriaceae Part 2 and Pseudo2023.Alex AlexNo ratings yet
- Nephritis Case: Understanding the PathogenesisDocument4 pagesNephritis Case: Understanding the PathogenesisEryll Paolo AleaNo ratings yet
- Intestinal Parasitism: ProtozoansDocument10 pagesIntestinal Parasitism: ProtozoansdtimtimanNo ratings yet
- Odessa National Medical University: Surgical InfectionsDocument34 pagesOdessa National Medical University: Surgical InfectionsDrRajneesh ShastriNo ratings yet
- Chapter 14-15, All Tables and Figures Taken From This ChapterDocument74 pagesChapter 14-15, All Tables and Figures Taken From This ChapterNour MohammedNo ratings yet
- J Clin Pathol 1980 Brook 1099 101Document4 pagesJ Clin Pathol 1980 Brook 1099 101ysh_girlNo ratings yet
- Bacterial Sepsis: I. The Concept of SepsisDocument8 pagesBacterial Sepsis: I. The Concept of SepsisIsra BalyNo ratings yet
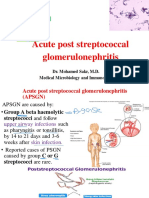
- Micro PSGNDocument32 pagesMicro PSGNMahmoud hilmyNo ratings yet
- Bacterial Infection On Respiration Tract: Ike Irmawati P.A, Msi Med Mikrobiologi FK YarsiDocument39 pagesBacterial Infection On Respiration Tract: Ike Irmawati P.A, Msi Med Mikrobiologi FK YarsiCamila SuhendarNo ratings yet
- True Bacteria - Cocci-Gram Positive Cocci Streptococci: Classification of StreptoccociDocument11 pagesTrue Bacteria - Cocci-Gram Positive Cocci Streptococci: Classification of StreptoccociSalimNo ratings yet
- Micro Chapter 17Document8 pagesMicro Chapter 17Ana AbuladzeNo ratings yet
- Partial of PathophysiologyDocument56 pagesPartial of Pathophysiologytoolsdesk1No ratings yet
- Demam Tifoid: Sigit Widyatmoko Fakultas Kedokteran Universitas Muhammadiyah SurakartaDocument37 pagesDemam Tifoid: Sigit Widyatmoko Fakultas Kedokteran Universitas Muhammadiyah SurakartasakyaNo ratings yet
- Amoebic Dysentery: Causes, Symptoms, and TreatmentDocument25 pagesAmoebic Dysentery: Causes, Symptoms, and TreatmentbebeweebeNo ratings yet
- Gram Negative Rods GuideDocument8 pagesGram Negative Rods GuideRuel Maddawin100% (1)
- Pleuropulmonary InfectionsDocument40 pagesPleuropulmonary InfectionsRahmidatul AftikaNo ratings yet
- Strep LectDocument35 pagesStrep LectAnne CabreraNo ratings yet
- Infectious Disease Pathology p31-55Document25 pagesInfectious Disease Pathology p31-55zeroun2450% (2)
- Typhoid FeverDocument9 pagesTyphoid FeverAli Al.JuffairiNo ratings yet
- Infectious Disease Pathology p56-75Document20 pagesInfectious Disease Pathology p56-75zeroun24No ratings yet
- Leptospirosis: Where Is Leptospirosis Found?Document4 pagesLeptospirosis: Where Is Leptospirosis Found?Ariffe Ad-dinNo ratings yet
- Clinical Bacteriology by DR Agwu EzeraDocument116 pagesClinical Bacteriology by DR Agwu EzeraRodgers Bazigu100% (1)
- NURSING CARE IN CHILDREN WITH TyphoidDocument26 pagesNURSING CARE IN CHILDREN WITH TyphoidKhabibahSaniyaRNo ratings yet
- Adult Still's Disease and Respiratory Failure in A 74 Year Old WomanDocument3 pagesAdult Still's Disease and Respiratory Failure in A 74 Year Old WomanEduardo Romero StéfaniNo ratings yet
- Case Report: Streptococcus AnginosusDocument4 pagesCase Report: Streptococcus AnginosusIesanu MaraNo ratings yet
- Upper Respiratory Tract Infections: DR John Egbagba FmcpathDocument37 pagesUpper Respiratory Tract Infections: DR John Egbagba FmcpathPrincewill SeiyefaNo ratings yet
- P.auroginosa and Bordetalla Pertusiss''''Document6 pagesP.auroginosa and Bordetalla Pertusiss''''Hisham ChomanyNo ratings yet
- Background: View Media GalleryDocument6 pagesBackground: View Media GalleryAlmas TNo ratings yet
- Intestinal Protozoa Amoebae & Ciliates: ObjectivesDocument5 pagesIntestinal Protozoa Amoebae & Ciliates: ObjectivesmicroperadeniyaNo ratings yet
- Plabable 2020 Infectious Disease BDRDocument69 pagesPlabable 2020 Infectious Disease BDRDr. Saqib RazaNo ratings yet
- Blood & CVSDocument64 pagesBlood & CVSNIVAAN S KNo ratings yet
- Neisseria, Diph, AnthraxDocument53 pagesNeisseria, Diph, AnthraxAyat MostafaNo ratings yet
- Bacillus SPP: There Are Two Medically ImportantDocument20 pagesBacillus SPP: There Are Two Medically ImportantEng CirroNo ratings yet
- Background: Ormdl3 and of GSDMB Were Significantly Increased in Hrv-Stimulated PBMCSDocument6 pagesBackground: Ormdl3 and of GSDMB Were Significantly Increased in Hrv-Stimulated PBMCSSav GaNo ratings yet
- Pathology MCQDocument9 pagesPathology MCQRashed Aiman Sameer Alsayyed Alalqamawi100% (1)
- SchistosomiasisDocument20 pagesSchistosomiasisAJAY MANDALNo ratings yet
- Lecture7 Medical Mycology - YeastsDocument32 pagesLecture7 Medical Mycology - YeastsKarthick AnbuNo ratings yet
- Bacillus and Biological Warfare: Dr. Samah Binte Latif M - Phil (Part-1), Microbiology Dhaka Medical CollegeDocument67 pagesBacillus and Biological Warfare: Dr. Samah Binte Latif M - Phil (Part-1), Microbiology Dhaka Medical CollegeTania.dmp20No ratings yet
- Acute appendicitis, pneumonia, tuberculosis and other medical quiz diagnosesDocument23 pagesAcute appendicitis, pneumonia, tuberculosis and other medical quiz diagnoses182 ROHIL HNo ratings yet
- Fundamentals of Colitis: Pergamon International Library of Science, Technology, Engineering and Social StudiesFrom EverandFundamentals of Colitis: Pergamon International Library of Science, Technology, Engineering and Social StudiesNo ratings yet
- ClinicoSocial Case on Household Assets and SanitationDocument9 pagesClinicoSocial Case on Household Assets and SanitationKalichandren ArumugamNo ratings yet
- EPSON L210 Series Advanced Driver SettingsDocument1 pageEPSON L210 Series Advanced Driver SettingsKalichandren ArumugamNo ratings yet
- Pro 3 Cases - Long and ShortDocument6 pagesPro 3 Cases - Long and ShortKalichandren ArumugamNo ratings yet
- SKILL LAB-HWS Relax TechniqueDocument2 pagesSKILL LAB-HWS Relax TechniqueKalichandren ArumugamNo ratings yet
- Year 3 October Intake - Rot 4time Table, 2015Document11 pagesYear 3 October Intake - Rot 4time Table, 2015Kalichandren ArumugamNo ratings yet
- Title Layout: SubtitleDocument11 pagesTitle Layout: SubtitleKalichandren ArumugamNo ratings yet
- EPSON L210 Series Advanced Driver SettingsDocument1 pageEPSON L210 Series Advanced Driver SettingsKalichandren ArumugamNo ratings yet
- GDocument17 pagesGKalichandren ArumugamNo ratings yet
- International Medical SchoolDocument1 pageInternational Medical SchoolKalichandren ArumugamNo ratings yet
- cp2 GRP BDocument35 pagescp2 GRP BKalichandren ArumugamNo ratings yet
- Presentation 4Document11 pagesPresentation 4Kalichandren ArumugamNo ratings yet
- Year 3 October Intake - Rot 4time Table, 2015Document11 pagesYear 3 October Intake - Rot 4time Table, 2015Kalichandren ArumugamNo ratings yet
- PresentationDocument1 pagePresentationAlexandra NeculaiNo ratings yet
- PresentationDocument1 pagePresentationAlexandra NeculaiNo ratings yet
- MnemonicDocument21 pagesMnemonicWiDya EmiLiaNo ratings yet
- Att List Mbbs Year 3 - Theory (5 June)Document176 pagesAtt List Mbbs Year 3 - Theory (5 June)Kalichandren ArumugamNo ratings yet
- Chest PainDocument7 pagesChest PainKalichandren ArumugamNo ratings yet
- 2Document17 pages2Kalichandren ArumugamNo ratings yet
- CardiovascularDocument8 pagesCardiovascularHampson MalekanoNo ratings yet
- Respi SystemDocument6 pagesRespi SystemKalichandren ArumugamNo ratings yet
- Spiro Me TryDocument22 pagesSpiro Me TryKalichandren ArumugamNo ratings yet
- Spiro Me TryDocument22 pagesSpiro Me TryKalichandren ArumugamNo ratings yet
- CPG Management of Type 2 Diabetes Mellitus (4th Edition)Document84 pagesCPG Management of Type 2 Diabetes Mellitus (4th Edition)apalaginih100% (3)
- CP 4Document79 pagesCP 4Kalichandren ArumugamNo ratings yet
- Chapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CDocument5 pagesChapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CKalichandren ArumugamNo ratings yet
- Chapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CDocument7 pagesChapter 71: Acute Gastroenteritis: Is The Child in Shock? Any Child With Shock Go Straight To Treatment Plan CKalichandren ArumugamNo ratings yet
- Year 3 - Learning OutcomeDocument8 pagesYear 3 - Learning OutcomeKalichandren ArumugamNo ratings yet
- CPG Medical StudentsDocument33 pagesCPG Medical StudentsKalichandren ArumugamNo ratings yet
- Groupon 4FA0D9B6F7Document1 pageGroupon 4FA0D9B6F7Kalichandren ArumugamNo ratings yet
- Forcep SeminarDocument3 pagesForcep SeminarKalichandren ArumugamNo ratings yet
- PEDIA Review TransesDocument12 pagesPEDIA Review TransesJennie KimNo ratings yet
- Care of The Mother, Child at Risk or With Problems (Acute and Chronic)Document6 pagesCare of The Mother, Child at Risk or With Problems (Acute and Chronic)Elizabeth ZamoraNo ratings yet
- Module 3 ReviDocument35 pagesModule 3 ReviJohn Van Dave TaturoNo ratings yet
- Fevers SeminarDocument20 pagesFevers Seminardagnenegash987No ratings yet
- MicrobiologyDocument20 pagesMicrobiologySarah JaneNo ratings yet
- Bpac Antibiotics Booklet PDFDocument20 pagesBpac Antibiotics Booklet PDFVenny Tri Pahlevi IINo ratings yet
- Science 9 Exemplar-Melc 2Document7 pagesScience 9 Exemplar-Melc 2Thartson Oliveros MagdadaroNo ratings yet
- Prevalence of Ventilator-Associated Pneumonia Among ICU Patients on VAP BundlesDocument33 pagesPrevalence of Ventilator-Associated Pneumonia Among ICU Patients on VAP BundlesGrace Cristobal PiggangayNo ratings yet
- Lung Patterns Made Easy (Proceedings) - DVM 360Document3 pagesLung Patterns Made Easy (Proceedings) - DVM 360dmantsioNo ratings yet
- Acute Prescribing - Challenges and Solutions - Ajit KulkarniDocument51 pagesAcute Prescribing - Challenges and Solutions - Ajit KulkarniAgha QaimiNo ratings yet
- Education and Practice: Approach To A Child With Recurrent PneumoniaDocument7 pagesEducation and Practice: Approach To A Child With Recurrent PneumoniaGd SuarantaNo ratings yet
- Klebsiella Pneumoniae TreatmentDocument2 pagesKlebsiella Pneumoniae Treatmentil_memoNo ratings yet
- Formulation Stabilisation and Encapsulation of Bacteriophage For Phage TherapyDocument34 pagesFormulation Stabilisation and Encapsulation of Bacteriophage For Phage TherapyGerman GodiNo ratings yet
- Tocilizumab and Remdesivir in HospitalizedDocument13 pagesTocilizumab and Remdesivir in HospitalizedYulian 53No ratings yet
- HemoptysisDocument35 pagesHemoptysisElad MizrahiNo ratings yet
- Full download book Textbook Of Critical Care Pdf pdfDocument41 pagesFull download book Textbook Of Critical Care Pdf pdfcharlotte.heckert523100% (15)
- InfectionDocument96 pagesInfectionBassem Georguos LabibNo ratings yet
- All India 2003Document55 pagesAll India 2003dhavalb20No ratings yet
- IFU Wondfo SARS CoV 2 Antibody Test (Lateral Flow Method) PDFDocument2 pagesIFU Wondfo SARS CoV 2 Antibody Test (Lateral Flow Method) PDFEndrio R HartonoNo ratings yet
- Upper Respiratory Tract InfectionDocument3 pagesUpper Respiratory Tract Infectionmcvirgo014100% (1)
- Common Respiratory Problems in Neonates & Infants 1Document46 pagesCommon Respiratory Problems in Neonates & Infants 1MichaelNo ratings yet
- Antibiotics Training ManualDocument149 pagesAntibiotics Training ManualImran MullaNo ratings yet
- CASE 2 PneumoniaDocument12 pagesCASE 2 PneumoniaKenneth MiguelNo ratings yet
- Imci DiscussionDocument147 pagesImci DiscussionPrisbert W. AlejoNo ratings yet
- Lung Disease: PneumoniaDocument2 pagesLung Disease: Pneumoniacayla mae carlosNo ratings yet
- Sputum Culture and SensitivityDocument8 pagesSputum Culture and SensitivityMarivic DianoNo ratings yet
- Nursing Care Plan for Pneumonia PatientDocument3 pagesNursing Care Plan for Pneumonia PatientRia LumacadNo ratings yet
- Kiara Denise Tamayo - MeaslesDocument3 pagesKiara Denise Tamayo - MeaslesKiara Denise TamayoNo ratings yet