You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Kraniotomi DekompresiDocument17 pagesKraniotomi DekompresianamselNo ratings yet
- 13fk10 Hav Igg-Igm (D) Ins (En) CeDocument2 pages13fk10 Hav Igg-Igm (D) Ins (En) CeCrcrjhjh RcrcjhjhNo ratings yet
- Ce Aduce Nou Interpretarea PolisomnografieDocument7 pagesCe Aduce Nou Interpretarea PolisomnografieLaura MoiseNo ratings yet
- Heart Sounds and MurmursDocument38 pagesHeart Sounds and MurmursLaura Moise100% (5)
- A Guide To Performing Quality Assured Diagnostic SpirometryDocument28 pagesA Guide To Performing Quality Assured Diagnostic SpirometryLaura MoiseNo ratings yet
- ATS ERS Spirometry Standards 2005Document20 pagesATS ERS Spirometry Standards 2005Laura MoiseNo ratings yet
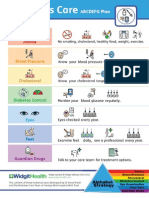
- Diabetes Alphabet Strategy SymbolsDocument9 pagesDiabetes Alphabet Strategy SymbolsLaura MoiseNo ratings yet
- Princess Mae S. ArellanoDocument2 pagesPrincess Mae S. ArellanoPrincess Mae ArellanoNo ratings yet
- Health and Safety at Work SlidesDocument195 pagesHealth and Safety at Work SlidesZulfiqar Hyder100% (2)
- EdCaN Specialty Module 4Document23 pagesEdCaN Specialty Module 4cindy8127No ratings yet
- O IntegratedscienceDocument36 pagesO IntegratedscienceFarai FaustosNo ratings yet
- 33 Pol BRF Food Models enDocument36 pages33 Pol BRF Food Models enthuyetnnNo ratings yet
- DM 2020-0187 - Must Know Covid IssuancesDocument18 pagesDM 2020-0187 - Must Know Covid IssuancesFranchise AlienNo ratings yet
- Omics Research Ethics ConsiderationsDocument26 pagesOmics Research Ethics ConsiderationsAndreea MadalinaNo ratings yet
- Nov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Document79 pagesNov 19 INTEGUMENTARY-INFLAMMATORY-DISORDERS-for-presentation-2022Jean Gwyneth GatchalianNo ratings yet
- Abg PalicDocument82 pagesAbg PalicHarry James PotterNo ratings yet
- NK 48InjuryCategoryPackagesDocument4 pagesNK 48InjuryCategoryPackagesJD Health Services TirupatturNo ratings yet
- Industrial SafetyDocument5 pagesIndustrial Safetykamujula reddyNo ratings yet
- Planning PlaygroundDocument16 pagesPlanning PlaygroundAdnan AliNo ratings yet
- Job Shadowing PresentationDocument12 pagesJob Shadowing Presentationapi-462381810No ratings yet
- 16-Week Harvey Walden MarathonTraining PlanDocument18 pages16-Week Harvey Walden MarathonTraining PlanKaren MiranoNo ratings yet
- WASH in CampsDocument13 pagesWASH in CampsMohammed AlfandiNo ratings yet
- Revised Week 3Document61 pagesRevised Week 3John Teo DalisaymoNo ratings yet
- The CSI Effect - Google FormsDocument12 pagesThe CSI Effect - Google FormsZivi DegenNo ratings yet
- 04fc75de986c12 Pharmaceutics-I AROMATIC WATERSDocument14 pages04fc75de986c12 Pharmaceutics-I AROMATIC WATERSsultanNo ratings yet
- BB - Self AuditDocument18 pagesBB - Self AuditFe Rackle Pisco JamerNo ratings yet
- 1.3.1 The Autopsy-1Document4 pages1.3.1 The Autopsy-1Alyssa robertsNo ratings yet
- Lepage Job WRKSHP 10-26-11Document2 pagesLepage Job WRKSHP 10-26-11Andi ParkinsonNo ratings yet
- EffectiveTeaching Full ManualDocument340 pagesEffectiveTeaching Full ManualHabtamu AdimasuNo ratings yet
- TES Harian: Bahasa InggrisDocument3 pagesTES Harian: Bahasa InggrisAlfiya HasnaNo ratings yet
- Training 11 Add 3 enDocument44 pagesTraining 11 Add 3 enBela CruzNo ratings yet
- 7 Contoh Analytical Exposition Pendek Bahasa InggrisDocument6 pages7 Contoh Analytical Exposition Pendek Bahasa InggrisDarsi YujiwatiNo ratings yet
- SAFed Tests PDFDocument88 pagesSAFed Tests PDFDanNo ratings yet
- Transform at Home EbookDocument302 pagesTransform at Home EbookLuckyNo ratings yet
- Sample Paper 1Document36 pagesSample Paper 1Annshai Jam MetanteNo ratings yet