You might also like
- NT BNPDocument9 pagesNT BNPSagar MhetreNo ratings yet
- Expression of The Nociceptin Precursor and NocicepDocument7 pagesExpression of The Nociceptin Precursor and NocicepRENAULTNo ratings yet
- Role of BNP and NT-proBNP in diagnosing heart failureDocument7 pagesRole of BNP and NT-proBNP in diagnosing heart failureyehezkieldwardNo ratings yet
- Utilizing Targeted Gene Therapy With Nano Particles Binding Alpha V Beta 3 For Imaging and Treating Choroidal NeovascularizationDocument9 pagesUtilizing Targeted Gene Therapy With Nano Particles Binding Alpha V Beta 3 For Imaging and Treating Choroidal Neovascularizationtennisboy92No ratings yet
- Pro BNP MetanalisisDocument30 pagesPro BNP MetanalisisOrkito Alvarez MontenegroNo ratings yet
- Protective Effect of 3-N-Butylphthalide Against Hypertensive Nephropathy in Spontaneously Hypertensive RatsDocument19 pagesProtective Effect of 3-N-Butylphthalide Against Hypertensive Nephropathy in Spontaneously Hypertensive Ratsberliana syifaNo ratings yet
- Tema 3 The Effect of Renal Dysfunction On BNP, NT-proBNPDocument10 pagesTema 3 The Effect of Renal Dysfunction On BNP, NT-proBNPRomaniuc IuliaNo ratings yet
- Ok 2012 CorrelationDocument3 pagesOk 2012 CorrelationsufaNo ratings yet
- Li 2004Document8 pagesLi 2004Shukr Wesman BlbasNo ratings yet
- NT proBNPDocument3 pagesNT proBNPTadilakshmikiranNo ratings yet
- BMM 2018 0348Document14 pagesBMM 2018 0348Harpreet SinghNo ratings yet
- Probnp II 2017-08 v12Document7 pagesProbnp II 2017-08 v12Yosef FerdinandNo ratings yet
- Gfy104 fp526Document1 pageGfy104 fp526spraptamaNo ratings yet
- Ni Hms 614459Document20 pagesNi Hms 614459Prakash GudsoorkarNo ratings yet
- Investigation Into The Use of Plasma Nt-Probnp Concentration To Screen For Feline Hypertrophic CardiomyopathyDocument8 pagesInvestigation Into The Use of Plasma Nt-Probnp Concentration To Screen For Feline Hypertrophic CardiomyopathyRoy SzeNo ratings yet
- 1 s2.0 S073510971636421X MainDocument12 pages1 s2.0 S073510971636421X Maincindy sitompulNo ratings yet
- Liver Stiffness As Measured by Transient Elastography - 2021 - American Heart JDocument6 pagesLiver Stiffness As Measured by Transient Elastography - 2021 - American Heart JGarret BarriNo ratings yet
- Bauch-Atrial Natriuretic Peptide As A MarDocument6 pagesBauch-Atrial Natriuretic Peptide As A MarSzendeNo ratings yet
- Phase 1b Trial of An Ibrutinib-Based Combination Therapy in Recurrent/refractory CNS LymphomaDocument6 pagesPhase 1b Trial of An Ibrutinib-Based Combination Therapy in Recurrent/refractory CNS LymphomaShiroNo ratings yet
- A Novel, Highly Sensitive and Specific Biomarker For Niemann-Pick Type C1 DiseaseDocument8 pagesA Novel, Highly Sensitive and Specific Biomarker For Niemann-Pick Type C1 DiseaseTheodora TeddyNo ratings yet
- Contribution of Speckle Tracking To Estimation of Pulmonary Hypertension by Standard Doppler Echocardiography in Patients With Sys 2161 1149 1000213Document5 pagesContribution of Speckle Tracking To Estimation of Pulmonary Hypertension by Standard Doppler Echocardiography in Patients With Sys 2161 1149 1000213a f indra pratamaNo ratings yet
- Pi Is 0973688315002650Document1 pagePi Is 0973688315002650ella faotNo ratings yet
- Cardiovascular Pleiotropic Effects of NUPDocument18 pagesCardiovascular Pleiotropic Effects of NUPВладимир ДружининNo ratings yet
- 1061 FullDocument7 pages1061 FullivanfreireNo ratings yet
- Introduction and aims of cardiovascular biomarker thesisDocument12 pagesIntroduction and aims of cardiovascular biomarker thesisRitendra TalapatraNo ratings yet
- 10 1111@ane 13078 PDFDocument17 pages10 1111@ane 13078 PDFFelipe MNo ratings yet
- Guide to BNP, a Heart HormoneDocument9 pagesGuide to BNP, a Heart HormoneRio Kristian NugrohoNo ratings yet
- Arn de InterferenciaDocument8 pagesArn de InterferenciaRosita Aguirre FloresNo ratings yet
- Ijms 20 03991Document7 pagesIjms 20 03991stevenburrow06No ratings yet
- Anastomosis Vol 1 Issue 2 PDFDocument36 pagesAnastomosis Vol 1 Issue 2 PDFRashin PNo ratings yet
- Nt-Probnp: The Gold Standard Biomarker in Heart FailureDocument3 pagesNt-Probnp: The Gold Standard Biomarker in Heart FailureRiuin23No ratings yet
- NPC1L1 Associated With Modest Alterations in Plasma LDL Cholesterol LevelsDocument8 pagesNPC1L1 Associated With Modest Alterations in Plasma LDL Cholesterol Levelsalexutzam09No ratings yet
- BNP in CKDDocument6 pagesBNP in CKDDedy ShauqiNo ratings yet
- MetabolismDocument8 pagesMetabolismMaria Ximena SilvaNo ratings yet
- 2013 Article 788Document5 pages2013 Article 788skripsi kapNo ratings yet
- OriginalDocument6 pagesOriginalSynder Castellanos del AguilaNo ratings yet
- Norepinephrine Kinetics and Dynamics in Septic Shock and Trauma PatientsDocument7 pagesNorepinephrine Kinetics and Dynamics in Septic Shock and Trauma PatientsMoh SuriyawalNo ratings yet
- Full Text 01Document6 pagesFull Text 01subhadutta769No ratings yet
- 36814803Document5 pages36814803Fernando CardiologíaNo ratings yet
- Oamjms 10b 1047Document5 pagesOamjms 10b 1047Sari RakhmawatiNo ratings yet
- Child Turcotte Pugh: Correlation Between Neutrophil To Lymphocyte Ratio With in Liver Cirrhosis PatientsDocument8 pagesChild Turcotte Pugh: Correlation Between Neutrophil To Lymphocyte Ratio With in Liver Cirrhosis PatientsainunnadzNo ratings yet
- BNP 3Document9 pagesBNP 3omarfaridtawfikNo ratings yet
- Misra 2012Document7 pagesMisra 2012Carlos RiquelmeNo ratings yet
- High Throughput GenotypingDocument8 pagesHigh Throughput GenotypingAmira RanicaNo ratings yet
- Admin,+47 Ism.v10i3.382 PDFDocument5 pagesAdmin,+47 Ism.v10i3.382 PDFIntan Ratu DNo ratings yet
- The Expression of Annexin II and Its Role in The Fibrinolytic Activity in Acute Promyelocytic LeukemiaDocument6 pagesThe Expression of Annexin II and Its Role in The Fibrinolytic Activity in Acute Promyelocytic LeukemiaLaura LópezNo ratings yet
- Brain Natriuretic PeptideDocument8 pagesBrain Natriuretic PeptidegunawanNo ratings yet
- A Novel Prothrombin Time Method To Measure All Non Vitamin K Dependent Oral Anticoagulants NOACsDocument7 pagesA Novel Prothrombin Time Method To Measure All Non Vitamin K Dependent Oral Anticoagulants NOACstaufik.abdiNo ratings yet
- Investigation of The Etiology of Anemia in Thromboangiitis ObliteransDocument6 pagesInvestigation of The Etiology of Anemia in Thromboangiitis ObliteransHusni mubarakNo ratings yet
- N-Terminal Pro-Brain Natriuretic Peptide Monoclonal - Dimension - Rev H DXDCM 09017fe980338ff4-1705666298857Document21 pagesN-Terminal Pro-Brain Natriuretic Peptide Monoclonal - Dimension - Rev H DXDCM 09017fe980338ff4-1705666298857Toni QuesadaNo ratings yet
- Pone 0165567Document14 pagesPone 0165567Pawan MishraNo ratings yet
- Diagnostic Accuracy of Pleural Fluid NT-Pro BNPDocument11 pagesDiagnostic Accuracy of Pleural Fluid NT-Pro BNPElteyb Nor eldaimNo ratings yet
- HK 3Document6 pagesHK 3gekayuuNo ratings yet
- New ResearchDocument6 pagesNew ResearchChloe MirandaNo ratings yet
- Clinical ResearchDocument13 pagesClinical ResearchkarmilaNo ratings yet
- BNP No Choque Geral 2015Document6 pagesBNP No Choque Geral 2015Débora AlvesNo ratings yet
- Pluripotent Anti-Inflammatory Immunomodulatory Effects of Papaverine Against Cerebral Ischemic-Reperfusion InjuryDocument23 pagesPluripotent Anti-Inflammatory Immunomodulatory Effects of Papaverine Against Cerebral Ischemic-Reperfusion InjuryDragomir MirunaNo ratings yet
- Int J Lab Hematology - 2022 - Marinov - Validation of A Single Tube 3 Colour Immature Red Blood Cell Screening Assay ForDocument7 pagesInt J Lab Hematology - 2022 - Marinov - Validation of A Single Tube 3 Colour Immature Red Blood Cell Screening Assay ForMaria SousaNo ratings yet
- PCR PublishedDocument8 pagesPCR PublishedMotikooNo ratings yet
- 68th AACC Annual Scientific Meeting Abstract eBookFrom Everand68th AACC Annual Scientific Meeting Abstract eBookNo ratings yet
- P8 Carrivick - Anti-Mullerian Hormone Stability - Effects of Temperature and TimeDocument1 pageP8 Carrivick - Anti-Mullerian Hormone Stability - Effects of Temperature and TimeYondri Mandaku TasidjawaNo ratings yet
- Protein Metabolism: Department of Biochemistry Medical Faculti of Hasanuddin UniversityDocument80 pagesProtein Metabolism: Department of Biochemistry Medical Faculti of Hasanuddin UniversityYondri Mandaku TasidjawaNo ratings yet
- Bio Identical VitaminsDocument24 pagesBio Identical VitaminshamzaloNo ratings yet
- Laparoscopic Sleeve Gastrectomy: Perioperative Outcomes, Weight Loss and Impact On Type 2 Diabetes Mellitus Over 2 YearsDocument5 pagesLaparoscopic Sleeve Gastrectomy: Perioperative Outcomes, Weight Loss and Impact On Type 2 Diabetes Mellitus Over 2 YearsYondri Mandaku TasidjawaNo ratings yet
- Pato Fisiologi Kuliah 4 TemperatureDocument16 pagesPato Fisiologi Kuliah 4 TemperatureYondri Mandaku TasidjawaNo ratings yet
- Red Wine and Diabetes Health: Getting Skin in The Game: R. Paul RobertsonDocument8 pagesRed Wine and Diabetes Health: Getting Skin in The Game: R. Paul RobertsonYondri Mandaku TasidjawaNo ratings yet
- Blood Bank Lab WorksheetDocument1 pageBlood Bank Lab WorksheetYondri Mandaku TasidjawaNo ratings yet
- Cell Base Model of HaemostasisDocument25 pagesCell Base Model of HaemostasisYondri Mandaku TasidjawaNo ratings yet
- Detection IHCDocument129 pagesDetection IHCYondri Mandaku TasidjawaNo ratings yet
- Urin 1Document10 pagesUrin 1Mardatillah WiranataNo ratings yet
- All About AnorexiaDocument19 pagesAll About Anorexiajdthx4uNo ratings yet
- Haider Study (2 PerhidrosisDocument7 pagesHaider Study (2 PerhidrosisYondri Mandaku TasidjawaNo ratings yet
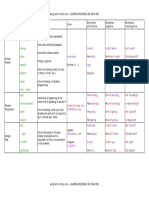
- Tenses Table PDFDocument5 pagesTenses Table PDFAlejandra Neira GonzálezNo ratings yet
- Artigo 13 - DM GestacionalDocument8 pagesArtigo 13 - DM GestacionalfahlevyNo ratings yet
- Print 1Document11 pagesPrint 1Yondri Mandaku TasidjawaNo ratings yet
- ADA Standards of Medical Care 2013 FINAL 21 Dec 2012Document146 pagesADA Standards of Medical Care 2013 FINAL 21 Dec 2012Mike MythiasNo ratings yet
- Nutrients 04 00208 v2Document23 pagesNutrients 04 00208 v2Yondri Mandaku TasidjawaNo ratings yet
- Critical Evaluation of Diagnosis and Outcomes of Gestational DiabetesDocument23 pagesCritical Evaluation of Diagnosis and Outcomes of Gestational DiabetesYondri Mandaku TasidjawaNo ratings yet
- Nutrients: The Potential Role of Vitamin D Enhanced Foods in Improving Vitamin D StatusDocument19 pagesNutrients: The Potential Role of Vitamin D Enhanced Foods in Improving Vitamin D StatusYondri Mandaku TasidjawaNo ratings yet
- 260 FullDocument7 pages260 FullYondri Mandaku TasidjawaNo ratings yet
- Healing Power of Sunlight and Witamin DDocument26 pagesHealing Power of Sunlight and Witamin Djecan100% (1)
- D-Vitamin PLOS OneDocument7 pagesD-Vitamin PLOS OneYondri Mandaku TasidjawaNo ratings yet
- GDM PresetationDocument26 pagesGDM PresetationYondri Mandaku TasidjawaNo ratings yet
- Ijo 201233 ADocument8 pagesIjo 201233 AYondri Mandaku TasidjawaNo ratings yet
- Curva ROC Metabolk-PasienDocument1 pageCurva ROC Metabolk-PasienYondri Mandaku TasidjawaNo ratings yet
- Aus Anorexia Nervosa PDFDocument31 pagesAus Anorexia Nervosa PDFYondri Mandaku Tasidjawa100% (1)
- 2147 FullDocument8 pages2147 FullYondri Mandaku TasidjawaNo ratings yet
- Aus Anorexia Nervosa PDFDocument31 pagesAus Anorexia Nervosa PDFYondri Mandaku Tasidjawa100% (1)
- Duvvuri2009AnorexiaNervosa PDFDocument8 pagesDuvvuri2009AnorexiaNervosa PDFYondri Mandaku TasidjawaNo ratings yet
- CSI Chennai 2016 Highlights PDFDocument190 pagesCSI Chennai 2016 Highlights PDFmohamedsmnNo ratings yet
- Natriuretic Peptide Measurement in NonDocument2 pagesNatriuretic Peptide Measurement in NonAde YonataNo ratings yet
- Elecsys Reference RangesDocument95 pagesElecsys Reference Rangescandy jmzNo ratings yet
- Cardiac biomarkers: cTnI and NT-proBNPDocument5 pagesCardiac biomarkers: cTnI and NT-proBNPAntonio SessaNo ratings yet
- Echo Heart FailureDocument82 pagesEcho Heart FailureJing CruzNo ratings yet
- Review: Clinical Chemistry 67:7 947-958 (2021)Document12 pagesReview: Clinical Chemistry 67:7 947-958 (2021)Genesis PerezNo ratings yet
- Cobas h232 Primary Care BrochureDocument12 pagesCobas h232 Primary Care Brochurerizal_aspanNo ratings yet
- 2022 Non-Cardiac SurgeryDocument105 pages2022 Non-Cardiac Surgeryhosameldin ahmedNo ratings yet
- Comparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsDocument54 pagesComparative Study of Serum and Biliary Lipid Profile in Libyan Gallstone PatientsJagannadha Rao PeelaNo ratings yet
- Tema 3 The Effect of Renal Dysfunction On BNP, NT-proBNPDocument10 pagesTema 3 The Effect of Renal Dysfunction On BNP, NT-proBNPRomaniuc IuliaNo ratings yet
- STRONG-HF TrialDocument16 pagesSTRONG-HF TrialyukeNo ratings yet
- Infinosis NT-proBNP IN047705 enDocument2 pagesInfinosis NT-proBNP IN047705 enMeditech visionbdNo ratings yet
- Accurate cardiac biomarker screening for catsDocument36 pagesAccurate cardiac biomarker screening for catsdmantsioNo ratings yet