You might also like
- ABC AbdomenDocument57 pagesABC AbdomenSyahmi KhalidNo ratings yet
- The Thoracic Outlet Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandThe Thoracic Outlet Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Periphral Vascular Disease 2Document44 pagesPeriphral Vascular Disease 2Sohil ElfarNo ratings yet
- Blunt Adominal TraumaDocument14 pagesBlunt Adominal TraumaMuhammad Bima AkbarNo ratings yet
- Diabetic Foot Assessment and Treatment ProtocolsDocument68 pagesDiabetic Foot Assessment and Treatment ProtocolsEndro Ri WibowoNo ratings yet
- Abdomen Injury-Dr - SayedDocument48 pagesAbdomen Injury-Dr - SayedAnonymous xmw6mrNo ratings yet
- New Approaches For The Treatment of Varicose Veins: Theodore H. Teruya, MD, FACS, Jeffrey L. Ballard, MD, FACSDocument21 pagesNew Approaches For The Treatment of Varicose Veins: Theodore H. Teruya, MD, FACS, Jeffrey L. Ballard, MD, FACSArturo Javier FuentesNo ratings yet
- Vascular Disease Approach 11-7-13Document65 pagesVascular Disease Approach 11-7-13Dian PuspaNo ratings yet
- Penetrating Abdominal TraumaDocument3 pagesPenetrating Abdominal TraumaamrulNo ratings yet
- Vascular Malformations Part IIDocument24 pagesVascular Malformations Part IIJuan RomeroNo ratings yet
- Vascular Note by Joel ArudchelvamDocument52 pagesVascular Note by Joel ArudchelvamJoel Arudchelvam100% (1)
- Updated review of diagnosis and treatment of cystic hepatic lesionsDocument8 pagesUpdated review of diagnosis and treatment of cystic hepatic lesionsMayerlin CalvacheNo ratings yet
- Vascular NotesDocument37 pagesVascular NotesAhmad SobihNo ratings yet
- Venous DiseaseDocument50 pagesVenous Diseasesgod34No ratings yet
- Postcholecystectomy SyndromeDocument27 pagesPostcholecystectomy SyndromeMonica TurnerNo ratings yet
- Retroperitoneal and Soft TissueDocument59 pagesRetroperitoneal and Soft TissueLucas Phi100% (1)
- Surgical Safety ChecklistDocument2 pagesSurgical Safety ChecklistLian CatindigNo ratings yet
- Diagnosis, Treatment and Follow-Up in Extracranial Carotid Stenosis, 2020Document16 pagesDiagnosis, Treatment and Follow-Up in Extracranial Carotid Stenosis, 2020CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- TRAUMA ORGAN ABDOMEN: ASSESSMENT AND MANAGEMENT OF BLUNT AND PENETRATING ABDOMINAL TRAUMADocument47 pagesTRAUMA ORGAN ABDOMEN: ASSESSMENT AND MANAGEMENT OF BLUNT AND PENETRATING ABDOMINAL TRAUMAreginaNo ratings yet
- Sinus, FistulaDocument46 pagesSinus, Fistulaalia0% (1)
- LiverDocument27 pagesLiverAndi Arwan AgusnawanNo ratings yet
- Surgery BookDocument95 pagesSurgery BookKhaled Mahmud100% (1)
- Intra Abdominal 2009Document8 pagesIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoNo ratings yet
- INGUINAL-SCROTAL SWELLINGS GUIDEDocument23 pagesINGUINAL-SCROTAL SWELLINGS GUIDEAzmyza Azmy100% (1)
- Remove clothing, log roll, expose entire body, maintain spinal precautions and warmthDocument29 pagesRemove clothing, log roll, expose entire body, maintain spinal precautions and warmthAjay DherwaniNo ratings yet
- Urogenital TumorDocument71 pagesUrogenital TumorJanet UngNo ratings yet
- Endovascular Surgery - BenkőDocument33 pagesEndovascular Surgery - BenkőpampaszNo ratings yet
- Corrosive Injury 20061227-1Document23 pagesCorrosive Injury 20061227-1ostaz2000No ratings yet
- Vascular Injury ManagementDocument53 pagesVascular Injury ManagementWiwin RahayuNo ratings yet
- Amputation in Lower LimbsDocument35 pagesAmputation in Lower LimbsSamNo ratings yet
- Esophagus CAP ProtocolDocument12 pagesEsophagus CAP ProtocolMichael Herman ChuiNo ratings yet
- History Taking in Urology-UndergraduateDocument12 pagesHistory Taking in Urology-Undergraduateasmaaburas100% (1)
- Vascular Presentation - Visceral Artery Aneurysms - MCGDocument22 pagesVascular Presentation - Visceral Artery Aneurysms - MCGYasir BouchiNo ratings yet
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADocument31 pagesIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangNo ratings yet
- Anal ProblemsDocument35 pagesAnal ProblemsSandip VaghelaNo ratings yet
- Chronic Venous Insufficiency - (Cvi)Document48 pagesChronic Venous Insufficiency - (Cvi)Andrei EfremovNo ratings yet
- IVUS Image GuideDocument17 pagesIVUS Image GuideRajesh JayakumarNo ratings yet
- Management of Trauma PatientDocument18 pagesManagement of Trauma PatientZahir MughalNo ratings yet
- NCCN HCC For Patients 2020Document76 pagesNCCN HCC For Patients 2020Dona LagurinNo ratings yet
- HemostasisDocument28 pagesHemostasisAkhmad MustafaNo ratings yet
- Abdominal Aortic AneurysmDocument1 pageAbdominal Aortic AneurysmIron ForceNo ratings yet
- Step2 Cs DDX and SymptomsDocument8 pagesStep2 Cs DDX and Symptomswalt65No ratings yet
- Vascular Sugergy Questions NasirDocument19 pagesVascular Sugergy Questions NasirAhmad SobihNo ratings yet
- Hanan Fathy Pediatric Nephrology Unit University of AlexandriaDocument47 pagesHanan Fathy Pediatric Nephrology Unit University of AlexandriadrhananfathyNo ratings yet
- Imaging in Vascular SurgeryDocument33 pagesImaging in Vascular Surgerydrzalie70100% (1)
- Rectal Cancer PPT 2.1Document131 pagesRectal Cancer PPT 2.1Usmle GuyNo ratings yet
- Radiology of The Urinary SystemDocument78 pagesRadiology of The Urinary Systemapi-19916399No ratings yet
- Vein Ligation and StrippingDocument4 pagesVein Ligation and StrippingNiken Feladita SantosoNo ratings yet
- Absite CH 32 BilliaryDocument14 pagesAbsite CH 32 BilliaryJames JosephNo ratings yet
- The European Trauma Course Manual: Edition 4.0Document10 pagesThe European Trauma Course Manual: Edition 4.0Ghenea Catalin-StefanNo ratings yet
- Aetiology, Pathology and Management of Enterocutaneous FistulaDocument34 pagesAetiology, Pathology and Management of Enterocutaneous Fistularoselinekhadija100% (1)
- Management of The Pancreatic Remnant During Whipple OperationDocument4 pagesManagement of The Pancreatic Remnant During Whipple OperationYacine Tarik Aizel100% (1)
- Bowel AnastomosisDocument30 pagesBowel AnastomosismrashaiedehNo ratings yet
- Spleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementDocument53 pagesSpleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementMuhammad SaadNo ratings yet
- PR BleedDocument20 pagesPR BleedCathy KayNo ratings yet
- Vascular Trauma: Badr Aljabri, MD, FRCSCDocument35 pagesVascular Trauma: Badr Aljabri, MD, FRCSCIndah Putri NingsihNo ratings yet
- Advances in Surgical NutritionDocument11 pagesAdvances in Surgical NutritionOtto Guillermo SontayNo ratings yet
- Urological EmergencyDocument83 pagesUrological EmergencyIrwan SaputraNo ratings yet
- C 1+ 2 Surgicl Pathology of OesophagusDocument91 pagesC 1+ 2 Surgicl Pathology of OesophagusSayuridark5No ratings yet
- Evaluation FormDocument2 pagesEvaluation Formcharity kalinowskyNo ratings yet
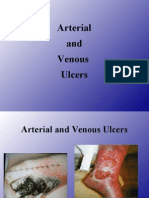
- 4 - Arterial & Venous UlcersDocument86 pages4 - Arterial & Venous Ulcerscharity kalinowsky100% (13)
- Metastatic WoundsDocument112 pagesMetastatic Woundscharity kalinowsky100% (1)
- 2 - Pressure UlcersDocument64 pages2 - Pressure Ulcerscharity kalinowsky100% (5)
- Treat The Cause, Patient/Family and The Wound A Combination That Can Prove DifficultDocument33 pagesTreat The Cause, Patient/Family and The Wound A Combination That Can Prove Difficultcharity kalinowskyNo ratings yet
- Ac PolypDocument18 pagesAc PolypSusmi CmNo ratings yet
- Surat Izin Masuk: FM.01-AOP - ROM/Rev.4.0/29.01.2020Document4 pagesSurat Izin Masuk: FM.01-AOP - ROM/Rev.4.0/29.01.2020Donking ThotosikNo ratings yet
- Sefcik Ashley Resume 2018Document1 pageSefcik Ashley Resume 2018api-394215168No ratings yet
- Procedure ListDocument20 pagesProcedure ListsoyrolandoNo ratings yet
- Revised Market Potential Estimates for Biopure's Hemopure Based on Competitive LandscapeDocument4 pagesRevised Market Potential Estimates for Biopure's Hemopure Based on Competitive Landscapeargand_xw9097No ratings yet
- Eucalyptus The Genus Eucalyptus PDFDocument433 pagesEucalyptus The Genus Eucalyptus PDFPeter Wilhelmsen100% (5)
- Melanoma Cancer PresentationDocument13 pagesMelanoma Cancer PresentationMerlyn JeejoNo ratings yet
- Drug Control Policy of BangladeshDocument51 pagesDrug Control Policy of BangladeshHedayat Ullah33% (3)
- End users' contact and product informationDocument3 pagesEnd users' contact and product informationمحمد ہاشمNo ratings yet
- CSOM of Middle Ear Part 2Document55 pagesCSOM of Middle Ear Part 2Anindya NandiNo ratings yet
- 837 Institutional 5010 PDFDocument610 pages837 Institutional 5010 PDFtrkreddyNo ratings yet
- Estradiol Valerate + Dienogest PDFDocument6 pagesEstradiol Valerate + Dienogest PDFJuan FernandezNo ratings yet
- Endocrine Exam ReviewDocument2 pagesEndocrine Exam Reviewrockforj3susNo ratings yet
- Sankar Ganguly - Pharma ManagerDocument2 pagesSankar Ganguly - Pharma Managersurojitsaha15094No ratings yet
- Dengulata KosamDocument3 pagesDengulata KosamChina SaidaNo ratings yet
- A Novel Visual Clue For The Diagnosis of Hypertrophic Lichen PlanusDocument1 pageA Novel Visual Clue For The Diagnosis of Hypertrophic Lichen Planus600WPMPONo ratings yet
- Tilapia 4Document69 pagesTilapia 4Annisa MeilaniNo ratings yet
- TEMPLATE-B-Master-list-of-Learners-for-the-Pilot-Implementation-of-F2F-Classes-for-S.Y.-2021-2022Document7 pagesTEMPLATE-B-Master-list-of-Learners-for-the-Pilot-Implementation-of-F2F-Classes-for-S.Y.-2021-2022Resa Consigna MagusaraNo ratings yet
- Phase 1 Mixed - MCQDocument74 pagesPhase 1 Mixed - MCQLee June LyngNo ratings yet
- Ifrs Issues Solutions For PharmaDocument109 pagesIfrs Issues Solutions For PharmaSrinivasa Rao100% (1)
- Healing Stories of People Final EditingDocument53 pagesHealing Stories of People Final Editinggabyk6867% (3)
- Radial Club Hand TreatmentDocument4 pagesRadial Club Hand TreatmentAshu AshNo ratings yet
- Class III Cavity Treatment (Procedure, Materials)Document2 pagesClass III Cavity Treatment (Procedure, Materials)Manos KritikosNo ratings yet
- Assignment On PrionsDocument22 pagesAssignment On PrionsRinta Moon100% (2)
- Voice Production in Singing and SpeakingBased On Scientific Principles (Fourth Edition, Revised and Enlarged) by Mills, Wesley, 1847-1915Document165 pagesVoice Production in Singing and SpeakingBased On Scientific Principles (Fourth Edition, Revised and Enlarged) by Mills, Wesley, 1847-1915Gutenberg.org100% (3)
- ICU HandoverDocument2 pagesICU HandoverMark 'Mark Douglas' DouglasNo ratings yet
- Antenatal & Postnatal Care: 1. General InformationDocument7 pagesAntenatal & Postnatal Care: 1. General InformationanishnithaNo ratings yet
- Chapter 6 DiscussionDocument3 pagesChapter 6 DiscussionyughaNo ratings yet
- KENCAP Changzhou 2013Document19 pagesKENCAP Changzhou 2013KencapchangzhouNo ratings yet
- 2014 Windsor University Commencement Ceremony PROOFDocument28 pages2014 Windsor University Commencement Ceremony PROOFKeidren LewiNo ratings yet