You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Optimum Theory of Population: An Assignment OnDocument10 pagesOptimum Theory of Population: An Assignment OnHarsh SenNo ratings yet
- Malaysia VBI Full ReportDocument116 pagesMalaysia VBI Full ReportHasoNo ratings yet
- Training Evaluation Form: Seven Seas HotelDocument2 pagesTraining Evaluation Form: Seven Seas HotelPiyush SevenseasNo ratings yet
- Earth Subsystem: BiosphereDocument17 pagesEarth Subsystem: BiosphereRhiza Mae LaxNo ratings yet
- Project Presentation On Rocker Bogie Suspension System: Babu Banarasi Das Northern India Institute of Technology, LucknowDocument21 pagesProject Presentation On Rocker Bogie Suspension System: Babu Banarasi Das Northern India Institute of Technology, LucknowAnoop SinghNo ratings yet
- Math 1st CODocument6 pagesMath 1st COfloriejanedNo ratings yet
- SAQOL 39 Proxy Version Sr55z7Document5 pagesSAQOL 39 Proxy Version Sr55z7Fernanda VegaNo ratings yet
- DESIGN AND ANALYSIS OF HYDRAULIC POWERPACK AND PUMcalculationsDocument10 pagesDESIGN AND ANALYSIS OF HYDRAULIC POWERPACK AND PUMcalculationssubhasNo ratings yet
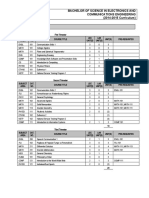
- Program Structure: Bachelor of Science in Electronics and Communications Engineering (2014-2015 Curriculum)Document5 pagesProgram Structure: Bachelor of Science in Electronics and Communications Engineering (2014-2015 Curriculum)Zainab KadhemNo ratings yet
- Sim2 Fads Vs Trends PDFDocument9 pagesSim2 Fads Vs Trends PDFMarciano MelchorNo ratings yet
- Veta 5 - Datasheet - ENG - 20210315Document3 pagesVeta 5 - Datasheet - ENG - 20210315JuanNo ratings yet
- A Level Physics Units & SymbolDocument3 pagesA Level Physics Units & SymbolXian Cong KoayNo ratings yet
- Executive MBA BrochureDocument36 pagesExecutive MBA BrochureAzad AMİROVNo ratings yet
- 1.3. Intention of This StudyDocument1 page1.3. Intention of This StudyJack FrostNo ratings yet
- Identification of The Best Model and Parameters For T-Y-X Equilibrium Data of Ethanol-Water MixtureDocument7 pagesIdentification of The Best Model and Parameters For T-Y-X Equilibrium Data of Ethanol-Water MixtureMeghana SNo ratings yet
- A12e IndicatorDocument2 pagesA12e IndicatorCyril J PadiyathNo ratings yet
- Mcdowell Review of Reverse Anthropology 19Document1 pageMcdowell Review of Reverse Anthropology 19PeriantroNo ratings yet
- Salt) Base) : Kantipur Engineering College Dhapakhel, LalitpurDocument3 pagesSalt) Base) : Kantipur Engineering College Dhapakhel, Lalitpursachin50% (2)
- Theory of Architecture 1 - ANTHROPOMETRY AND ERGONOMICSDocument1 pageTheory of Architecture 1 - ANTHROPOMETRY AND ERGONOMICSJHON MICCO ERGINANo ratings yet
- Cable For Solar Power SystemDocument1 pageCable For Solar Power SystemEnspartan 63No ratings yet
- Test Bank For Parent Child Relations Context Research and Application 4th by HeathDocument24 pagesTest Bank For Parent Child Relations Context Research and Application 4th by HeathMichaelNguyenwgok100% (44)
- Statisticsprobability11 q4 Week2 v4Document10 pagesStatisticsprobability11 q4 Week2 v4Sheryn CredoNo ratings yet
- Notes On Intertemporal Optimization: Econ 204A - Henning BohnDocument11 pagesNotes On Intertemporal Optimization: Econ 204A - Henning BohnHector RubiniNo ratings yet
- Histology SlidesDocument47 pagesHistology SlidesHaJoRaNo ratings yet
- Lesson 1 MATHEMATICS IN THE MODERN WORLDDocument39 pagesLesson 1 MATHEMATICS IN THE MODERN WORLDericacatu3No ratings yet
- Grundig Cuc4511Document68 pagesGrundig Cuc4511Saulius KalasauskasNo ratings yet
- ManualDocument272 pagesManualAkash AroraNo ratings yet
- ANNEX A. Integrated Planning ProcessDocument3 pagesANNEX A. Integrated Planning Processcarlito alvarezNo ratings yet
- Random Process Analysis With R Marco Bittelli All ChapterDocument67 pagesRandom Process Analysis With R Marco Bittelli All Chapterdorothy.rehberg545100% (3)
- MomentumDocument16 pagesMomentumminglei caiNo ratings yet