You might also like
- Pain Relief in Palliative Care, A Focus On Interventional Pain Management PDFDocument11 pagesPain Relief in Palliative Care, A Focus On Interventional Pain Management PDFShinichi Ferry RoferdiNo ratings yet
- Mechanism of Pain and Pain Management: Questions ANSWERS and Rationale ReferencesDocument23 pagesMechanism of Pain and Pain Management: Questions ANSWERS and Rationale ReferencesAngela Nicole LaredoNo ratings yet
- Low Back PainDocument34 pagesLow Back PainFAMED RESIDENTS CESMEDNo ratings yet
- Lumbar Herniated DiscDocument5 pagesLumbar Herniated DiscRinda AndreanditaNo ratings yet
- Schmitz2013 Article TreatmentOfChronicPlantarFasciDocument11 pagesSchmitz2013 Article TreatmentOfChronicPlantarFasciValeria GutiérrezNo ratings yet
- Management of Vertigo - DR - Attiya Rahma SpsDocument59 pagesManagement of Vertigo - DR - Attiya Rahma SpsHenni Pus Vera100% (1)
- A Patients Guide To Plantar Fasciitis Heel PainDocument4 pagesA Patients Guide To Plantar Fasciitis Heel PainJacobfranNo ratings yet
- Avascular NecrosisDocument8 pagesAvascular NecrosisBobyAnugrahNo ratings yet
- What Is Shock Wave Therap 2Document7 pagesWhat Is Shock Wave Therap 2api-457017927No ratings yet
- Eular Us Course Modulo 3 CotoveloDocument26 pagesEular Us Course Modulo 3 CotoveloGustavo Bernardo DamascenoNo ratings yet
- SPONDYLODISCITISDocument16 pagesSPONDYLODISCITISCitra Wulandari SofyanNo ratings yet
- Osteoarthritis of The KneeDocument8 pagesOsteoarthritis of The Kneeas3syamut649250% (2)
- All ThesisDocument113 pagesAll ThesisImraan KhanNo ratings yet
- Low Back PainDocument53 pagesLow Back PainSahara EffendyNo ratings yet
- Pyogenic Discitis Power PointDocument121 pagesPyogenic Discitis Power Pointjav_luv37No ratings yet
- Parkinsons DiseaseDocument14 pagesParkinsons DiseaseRia り あ HitsugayaNo ratings yet
- Lumbar Radicular Pain: PathophysiologyDocument4 pagesLumbar Radicular Pain: PathophysiologynetifarhatiiNo ratings yet
- TENSDocument20 pagesTENSchandran2679100% (2)
- Cancer PainDocument14 pagesCancer PainPratita Jati PermatasariNo ratings yet
- Introduction to Intervertebral Disc Anatomy and PIVD ManagementDocument104 pagesIntroduction to Intervertebral Disc Anatomy and PIVD ManagementVivek SaxenaNo ratings yet
- Pathophysiology of OsteoarthritisDocument2 pagesPathophysiology of OsteoarthritisRhia Maya SNo ratings yet
- Lipoma: Common Benign Fatty TumorsDocument9 pagesLipoma: Common Benign Fatty Tumorsshewasnot inrightmindNo ratings yet
- Carpal Tunnel Syndrome JAAOS 2007 PDFDocument12 pagesCarpal Tunnel Syndrome JAAOS 2007 PDFStefano Pareschi PasténNo ratings yet
- 2012-04-24 FK PainDocument49 pages2012-04-24 FK PainYanis Widhiya NingrumNo ratings yet
- Accese de astm bronsic-Dexametazon, Prednisolon,Adrenalin, Edemele gravidelor-furosemid, triamteren,amiloridDocument1 pageAccese de astm bronsic-Dexametazon, Prednisolon,Adrenalin, Edemele gravidelor-furosemid, triamteren,amiloridNatalia SpoialoNo ratings yet
- Platelet-Rich Plasma in Osteoarthritis Treatment: Review of Current EvidenceDocument18 pagesPlatelet-Rich Plasma in Osteoarthritis Treatment: Review of Current EvidenceIrham KhairiNo ratings yet
- Pain and SurgeryDocument15 pagesPain and SurgeryXinn Xinn Vanzandt100% (1)
- C TrialsDocument24 pagesC TrialsFauzi SebunyaNo ratings yet
- ActonelDocument42 pagesActonelSimon JonatanNo ratings yet
- The Hepatorenal SyndromeDocument26 pagesThe Hepatorenal SyndromeWaraBawanaNo ratings yet
- Ultrasound Guided Lower Limb Blocks Tony AllenDocument39 pagesUltrasound Guided Lower Limb Blocks Tony Allenrepre64No ratings yet
- Osteonecrosis of The Femoral Head: Kriangk BenjawongsathianDocument65 pagesOsteonecrosis of The Femoral Head: Kriangk Benjawongsathianryc0% (1)
- Exercitii ReabilitareDocument5 pagesExercitii ReabilitareGabriela Istrati-StanciugelNo ratings yet
- BMJ Summary of Cervical Spondylosis and Neck Pain TreatmentsDocument5 pagesBMJ Summary of Cervical Spondylosis and Neck Pain TreatmentsIsaac AlemanNo ratings yet
- 2016 The American Society of Shoulder and ElbowDocument15 pages2016 The American Society of Shoulder and ElbowDiego De Farias Diehl100% (1)
- WHO analgesic ladder three-step approachDocument2 pagesWHO analgesic ladder three-step approachAndi PakdheeNo ratings yet
- Chapter 10 - Trigeminal NeuralgiaDocument5 pagesChapter 10 - Trigeminal NeuralgiaMuhammad IkbarNo ratings yet
- Farmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiDocument19 pagesFarmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiCici MastaNo ratings yet
- The Anatomy Physiology PainDocument5 pagesThe Anatomy Physiology PaincrownesyaNo ratings yet
- Myotonometer ManualDocument30 pagesMyotonometer ManualRucsandra Avirvarei100% (1)
- c2Document37 pagesc2LuisAngelPonceTorresNo ratings yet
- A Case Study Utilizing Vojta Dynamic Neuromuscular Stabilization Therapy To Control Symptoms of A Chronic Migraine Sufferer 2011 Journal of Bodywork ADocument4 pagesA Case Study Utilizing Vojta Dynamic Neuromuscular Stabilization Therapy To Control Symptoms of A Chronic Migraine Sufferer 2011 Journal of Bodywork AJose J.No ratings yet
- LymphedemaDocument6 pagesLymphedemaPriyangga Rakatama100% (1)
- SpondilodiscytisDocument16 pagesSpondilodiscytischristinawiyaniputriNo ratings yet
- Muscle SpindlesDocument19 pagesMuscle SpindlesBenedek IldikoNo ratings yet
- Journal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDDocument9 pagesJournal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDWinda FRNo ratings yet
- Painful Hemiplegic ShoulderDocument53 pagesPainful Hemiplegic ShoulderpipitNo ratings yet
- Cancer Pain ManagementDocument48 pagesCancer Pain ManagementRifka Septia PutriNo ratings yet
- Myofascial Pain SyndromeDocument4 pagesMyofascial Pain SyndromeDusan OrescaninNo ratings yet
- Psoriatic ArthritisDocument12 pagesPsoriatic ArthritisSelvia RosadiNo ratings yet
- Dysfunction As Well, Both of Them Occuring in The Circuits ConnectingDocument25 pagesDysfunction As Well, Both of Them Occuring in The Circuits ConnectingRalucaNo ratings yet
- Carpal Tunnel SyndromeDocument2 pagesCarpal Tunnel Syndromeurkevet100% (1)
- Towards New Therapies For Parkinson's DiseaseDocument408 pagesTowards New Therapies For Parkinson's DiseaseAlexandra BalanNo ratings yet
- Degenerative Spinal DisordersDocument47 pagesDegenerative Spinal Disordersasad1912No ratings yet
- Spond I Lolis Tez IsDocument12 pagesSpond I Lolis Tez IsCosmin AlexaNo ratings yet
- Understanding Peripheral Neuropathic Pain in Primary Care: Diagnosis and ManagementDocument7 pagesUnderstanding Peripheral Neuropathic Pain in Primary Care: Diagnosis and ManagementInês Beatriz Clemente CasinhasNo ratings yet
- AliliDocument3 pagesAliliSaf Tanggo DiampuanNo ratings yet
- Anestesi Text Book ReadingDocument5 pagesAnestesi Text Book Readingli2delNo ratings yet
- Managing Neuropathic PainDocument10 pagesManaging Neuropathic PainAgusBhakti100% (1)
- OET Preparation Book Reading Sub Test Volume 1 Anna HartfordDocument131 pagesOET Preparation Book Reading Sub Test Volume 1 Anna HartfordASHITH86% (28)
- Aha Acsm Risk Screening AdaDocument1 pageAha Acsm Risk Screening AdawalterNo ratings yet
- Test Bank For Introduction To Medical Surgical Nursing 5th Edition LintonDocument36 pagesTest Bank For Introduction To Medical Surgical Nursing 5th Edition Lintonpatnesspertain.e2nd2o100% (44)
- Renal - MedbulletsDocument74 pagesRenal - Medbulletssmian08No ratings yet
- Radiology by Zainab VoraDocument19 pagesRadiology by Zainab VoraAnkit Tonger Anky100% (1)
- Harrisons Neurology in Clinical Medicine, 3E PDFDocument896 pagesHarrisons Neurology in Clinical Medicine, 3E PDFFelly Liu100% (7)
- Thyroid Disease in PregnancyDocument24 pagesThyroid Disease in PregnancyPanglimaNusantara100% (2)
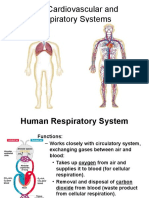
- Cardiovascular and Respiratory SystemDocument51 pagesCardiovascular and Respiratory SystemKarel Mae SanoriaNo ratings yet
- Dockong WebsiteDocument13 pagesDockong WebsitesripteraptorNo ratings yet
- Lung Summary LeafletDocument4 pagesLung Summary LeafletDev Ebenezer JohnsonNo ratings yet
- Newly Diagnosed and Relapsed Epithelial Ovarian CancerDocument16 pagesNewly Diagnosed and Relapsed Epithelial Ovarian CancerDragos VrancianuNo ratings yet
- Recent Advances in Applications of Multimodal Ultrasound-Guided Photoacoustic Imaging Technology-2020Document12 pagesRecent Advances in Applications of Multimodal Ultrasound-Guided Photoacoustic Imaging Technology-2020Elizabeth EspitiaNo ratings yet
- The Role of Shiatsu in The Treatment of The Side-EffectsDocument3 pagesThe Role of Shiatsu in The Treatment of The Side-Effectsapi-26008400No ratings yet
- Quiz With Answer and RationaleDocument4 pagesQuiz With Answer and Rationaleann aquinoNo ratings yet
- Pioped PDFDocument7 pagesPioped PDFaiNo ratings yet
- IAEA Tec28 PDFDocument61 pagesIAEA Tec28 PDFGezim HodolliNo ratings yet
- EXPERT DDX - Obstetrics - P. Woodward, Et. Al., (Amirsys, 2009) WW PDFDocument504 pagesEXPERT DDX - Obstetrics - P. Woodward, Et. Al., (Amirsys, 2009) WW PDFSebiUrzica100% (1)
- Gastric CancerDocument7 pagesGastric CancerMuhadis AhmadNo ratings yet
- Dental Implants in Diabetic PatientsDocument6 pagesDental Implants in Diabetic PatientsSilvia SoareNo ratings yet
- Approach To LymphadenopathyDocument55 pagesApproach To LymphadenopathyVaibhav KaroliyaNo ratings yet
- Haematology Diagnosis-Army USADocument205 pagesHaematology Diagnosis-Army USAManuela BotisNo ratings yet
- Barium MealDocument3 pagesBarium MealYusra Shafiq AhmedNo ratings yet
- AGICO Launches Pet InsuranceDocument7 pagesAGICO Launches Pet InsuranceZainab QayyumNo ratings yet
- NCPDocument2 pagesNCPJhel NabosNo ratings yet
- ICD-10 Volume 3Document842 pagesICD-10 Volume 3janki100% (1)
- Emergency Medicine MneumonicsDocument4 pagesEmergency Medicine Mneumonicsadwait marhattaNo ratings yet
- PG Diploma Courses TamilnaduDocument14 pagesPG Diploma Courses TamilnaduDENTALORG.COM100% (2)
- Chicago Electric Power Shears 92115Document14 pagesChicago Electric Power Shears 92115John SmithNo ratings yet
- Obstetrics MCQDocument8 pagesObstetrics MCQSandip Patil100% (6)
- Clinical MnemonicsDocument23 pagesClinical MnemonicsMing WangNo ratings yet