You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GEK 63383d Turbine Generator FoundationDocument61 pagesGEK 63383d Turbine Generator Foundationbong2rm100% (6)
- Group 1 Nondigital Instructional MaterialsDocument22 pagesGroup 1 Nondigital Instructional MaterialsJhon Paul Esplanada Soriano100% (1)
- Software Requirements Specification TemplateDocument6 pagesSoftware Requirements Specification TemplatekkrrrsssNo ratings yet
- Modeling of Deepwater-Type Rectangular Tuned Liquid Damper With Submerged NetsDocument10 pagesModeling of Deepwater-Type Rectangular Tuned Liquid Damper With Submerged NetsDhirendra Kumar PandeyNo ratings yet
- Poly Suga BetaineDocument4 pagesPoly Suga Betainemndmatt100% (1)
- Course On Fracture Mechanics - IIT RoparDocument248 pagesCourse On Fracture Mechanics - IIT RoparSumit BasuNo ratings yet
- C#Document3 pagesC#Dung RieuNo ratings yet
- Final Introduction To Community Based Management PowerpointDocument36 pagesFinal Introduction To Community Based Management PowerpointJazmine AlgerNo ratings yet
- A Framework For Engaging Diverse Communities in Citizen Science in The USDocument4 pagesA Framework For Engaging Diverse Communities in Citizen Science in The UStesemar010No ratings yet
- QSV 2 Product Release Procedure EN 01 PDFDocument6 pagesQSV 2 Product Release Procedure EN 01 PDFprashanthNo ratings yet
- EEG383 Measurement - Chapter 2 - Characteristics of Measuring InstrumentsDocument26 pagesEEG383 Measurement - Chapter 2 - Characteristics of Measuring Instrumentsايهاب غزالة100% (1)
- MD Nastran R3 - Explicit Nonlinear SOL 700 User's Guide PDFDocument602 pagesMD Nastran R3 - Explicit Nonlinear SOL 700 User's Guide PDFpezz07No ratings yet
- Welspun India LTD: AN Industrial Visit Report ONDocument12 pagesWelspun India LTD: AN Industrial Visit Report ONHitu100% (2)
- Physics Chapter 3 Practice TestDocument2 pagesPhysics Chapter 3 Practice TestVanessa Bugarin MananzanNo ratings yet
- WebSphere Application Server AMI Cheatsheet For DemoDocument2 pagesWebSphere Application Server AMI Cheatsheet For DemoYakura CoffeeNo ratings yet
- Simple Linear RegressionDocument55 pagesSimple Linear RegressionPatrick HernandezNo ratings yet
- Epilogue Magazine, March 2010Document56 pagesEpilogue Magazine, March 2010Epilogue MagazineNo ratings yet
- Renalyn N. Selloga Housekeeping NC IiDocument9 pagesRenalyn N. Selloga Housekeeping NC IiAlex GinNo ratings yet
- Action Research: Repeated Reading To Improve Students' Reading FluencyDocument4 pagesAction Research: Repeated Reading To Improve Students' Reading FluencyIylia NatasyaNo ratings yet
- Material SelectionDocument58 pagesMaterial SelectionSivareddy InduriNo ratings yet
- Shortcut To English CollocationDocument240 pagesShortcut To English Collocationtiago90% (10)
- The Art of Fishing PDFDocument27 pagesThe Art of Fishing PDFsilentkillersbh1729No ratings yet
- Hot Runner KEBA2580 220VDocument19 pagesHot Runner KEBA2580 220VAarón DíazNo ratings yet
- Spss 1. Uji Normalitas Data: One-Sample Kolmogorov-Smirnov TestDocument3 pagesSpss 1. Uji Normalitas Data: One-Sample Kolmogorov-Smirnov Testmustakim gmaNo ratings yet
- 1200單字分類表Document14 pages1200單字分類表joanne0049No ratings yet
- ThermodynamicsDocument60 pagesThermodynamicsMahender ThotakuriNo ratings yet
- 505xt 1 en PDFDocument242 pages505xt 1 en PDFSyed Mohammad NaveedNo ratings yet
- ELECTROSTATICSDocument21 pagesELECTROSTATICSHemanthNo ratings yet
- Lecture 9 - Symmetry & Concentricity, Expanded Position TolerancingDocument19 pagesLecture 9 - Symmetry & Concentricity, Expanded Position Tolerancingג'ון ירוקNo ratings yet
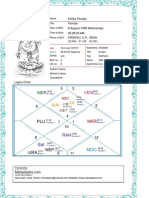
- Kritika Pandey (Kaushambi)Document15 pagesKritika Pandey (Kaushambi)nishink9No ratings yet