You might also like
- The Effects of Pre Anesthetic, Single-Dose Dexmedetomidine On Ion Hemodynamic and Cardiovascular ParametersDocument6 pagesThe Effects of Pre Anesthetic, Single-Dose Dexmedetomidine On Ion Hemodynamic and Cardiovascular ParametersjcaegNo ratings yet
- Pre MedicationDocument4 pagesPre MedicationjcaegNo ratings yet
- Pharmacology of Sedative Analgesic Agents DexmedetomidineDocument19 pagesPharmacology of Sedative Analgesic Agents DexmedetomidinejcaegNo ratings yet
- Monitoring Endocrine FunctionDocument10 pagesMonitoring Endocrine FunctionjcaegNo ratings yet
- Perioperative Fluid TherapyDocument3 pagesPerioperative Fluid Therapyjcaeg100% (1)
- Hormonal and Metabolic Responses To TraumaDocument3 pagesHormonal and Metabolic Responses To TraumajcaegNo ratings yet
- Fluid Therapy For The Surgical PatientDocument19 pagesFluid Therapy For The Surgical PatientjcaegNo ratings yet
- Dexmedetomidine As Sole Sedative For Awake Ion in Management of The Critical AirwayDocument4 pagesDexmedetomidine As Sole Sedative For Awake Ion in Management of The Critical AirwayjcaegNo ratings yet
- Pre MedicationDocument4 pagesPre MedicationjcaegNo ratings yet
- Clinical Aspects of EndocrinologyDocument4 pagesClinical Aspects of EndocrinologyjcaegNo ratings yet
- Anaesthesia For NeurosurgeryDocument4 pagesAnaesthesia For NeurosurgeryjcaegNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Thyroid Function Test ResultsDocument2 pagesThyroid Function Test ResultsFullOnNo ratings yet
- Meta Dbol CycleDocument4 pagesMeta Dbol CyclestuNo ratings yet
- Ispitna Pitanja Farmacija Medicinska BiohemijaDocument2 pagesIspitna Pitanja Farmacija Medicinska BiohemijaTijanaNo ratings yet
- Multiple-Choice QuizDocument6 pagesMultiple-Choice QuizHUAWEI HUAWEI100% (1)
- Adrenal Function TestDocument26 pagesAdrenal Function TestSaroja Veeresh83% (6)
- Lyphochek Immunoassay Plus Control Levels 1, 2 and 3: Revision Date 2020-06-29 Indicates Revised InformationDocument2 pagesLyphochek Immunoassay Plus Control Levels 1, 2 and 3: Revision Date 2020-06-29 Indicates Revised InformationMDD Engineering100% (2)
- IPF Sanction Registry 20220914Document3 pagesIPF Sanction Registry 20220914Ryan AuliaNo ratings yet
- Chap 5 Hormonal Response To ExerciseDocument53 pagesChap 5 Hormonal Response To ExerciseAnnie KhanNo ratings yet
- The Role of Hormones in HumanDocument2 pagesThe Role of Hormones in HumandebbycleyNo ratings yet
- Precocious PubertyDocument30 pagesPrecocious PubertyAjoritsedere Eric AkonuNo ratings yet
- Endocrine System: Name: - Class: - DateDocument7 pagesEndocrine System: Name: - Class: - DateKesithan AnandarashNo ratings yet
- Free delivery for orders over 500pln at Poland men's physique storeDocument1 pageFree delivery for orders over 500pln at Poland men's physique storesahilNo ratings yet
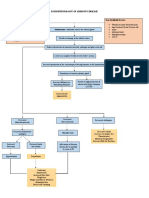
- Pathophysiology of Addison's Disease ExplainedDocument2 pagesPathophysiology of Addison's Disease ExplainedHanna NocumNo ratings yet
- Pregnant Woman's HCG, T4 and TSH Test ResultsDocument3 pagesPregnant Woman's HCG, T4 and TSH Test ResultsBALANo ratings yet
- AP13 EndocrineDocument12 pagesAP13 EndocrinePay per PrintNo ratings yet
- Male Androgens PDFDocument17 pagesMale Androgens PDFGreg RalphNo ratings yet
- AntiandrogensDocument22 pagesAntiandrogenstheintrovNo ratings yet
- MCQ REPRODUCTION: HORMONES, FOLLICULAR DEVELOPMENT, MENSTRUAL CYCLEDocument2 pagesMCQ REPRODUCTION: HORMONES, FOLLICULAR DEVELOPMENT, MENSTRUAL CYCLEwanderer_1010100% (1)
- Lyphochek Immunoassay Plus Control Levels 1, 2 and 3: Revision Date 2020-06-29 Indicates Revised InformationDocument2 pagesLyphochek Immunoassay Plus Control Levels 1, 2 and 3: Revision Date 2020-06-29 Indicates Revised InformationMDD Engineering100% (3)
- Anterior and Posterio Pituitary GlandDocument7 pagesAnterior and Posterio Pituitary GlandAnny AlvrzNo ratings yet
- Pituitary GlandDocument3 pagesPituitary GlandAllyza Marie PeñaNo ratings yet
- (Pha) Le 5Document19 pages(Pha) Le 5Gabby TanNo ratings yet
- Liquichek Immunoassay Plus Control Levels 1, 2 and 3: InstrumentoDocument2 pagesLiquichek Immunoassay Plus Control Levels 1, 2 and 3: InstrumentoMauricio VidalNo ratings yet
- CDGP Versus HypogonadismDocument25 pagesCDGP Versus HypogonadismmpintobNo ratings yet
- Thyroid Disease OutlineDocument3 pagesThyroid Disease OutlinePaige BarniniNo ratings yet
- Transport of HormonesDocument5 pagesTransport of HormonesJohn MusaNo ratings yet
- Hypothalamus Pituitary and Gonad AxisDocument6 pagesHypothalamus Pituitary and Gonad Axisalok nayakNo ratings yet
- Major and Minor Scale Fingerings for PianoDocument2 pagesMajor and Minor Scale Fingerings for PianoJames RileyNo ratings yet
- Dexamethasone Suppression TestDocument2 pagesDexamethasone Suppression Testjbeans92No ratings yet
- HormonesDocument29 pagesHormonesCandy Chieng67% (3)