Professional Documents
Culture Documents
S807 Mini Review v4
Uploaded by
Daen de LeonCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
S807 Mini Review v4
Uploaded by
Daen de LeonCopyright:
Available Formats
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
S807 Mini-Review
Cisplatin Resistance
Daen de Leon M3852083
September 15th 2002
Page 1 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
1 INTRODUCTION...........................................................................................................................................2
2 CANCER AND CISPLATIN..........................................................................................................................4
2.1 THE EUKARYOTIC CELL CYCLE ..................................................................................................................5
2.2 DNA REPAIR MECHANISMS ......................................................................................................................6
2.3 ADDUCT FORMATION................................................................................................................................7
2.4 CYTOTOXICITY ........................................................................................................................................8
3 MECHANISMS OF CISPLATIN RESISTANCE..........................................................................................10
3.1 DECREASED UPTAKE .............................................................................................................................11
3.2 INCREASED EFFLUX..............................................................................................................................12
3.3 GLUTATHIONE AND METALLOTHIONEIN INACTIVATION .......................................................................................13
3.4 INCREASED NUCLEOTIDE EXCISION REPAIR (NER)......................................................................................14
3.5 MISMATCH REPAIR MECHANISMS (MMR)..................................................................................................16
3.6 INCREASED ADDUCT TOLERANCE...............................................................................................................17
3.7 HOMOLOGOUS RECOMBINATION................................................................................................................18
3.8 REGULATORY PROTEINS.........................................................................................................................20
4 PROBLEMS OF INVESTIGATING CISPLATIN RESISTANCE.................................................................23
4.1 MULTIFACTORIAL NATURE OF CISPLATIN RESISTANCE.....................................................................................24
4.2 CELL LINES.........................................................................................................................................25
4.3 IN VIVO VS IN VITRO.............................................................................................................................27
5 PROSPECTS FOR INTERVENTION..........................................................................................................28
5.1 REPLACING CISPLATIN............................................................................................................................29
5.2 COMBINATION THERAPY WITH CISPLATIN.....................................................................................................30
5.3 OTHER APPROACHES .............................................................................................................................31
6 CONCLUSION............................................................................................................................................32
7 FIGURES & REFERENCES.......................................................................................................................33
1 Introduction
This review examines the mechanisms of resistance to cis-Diamminedichloroplatinum(II)
(cisplatin, cis-DDP or CDDP - see Fig. 1). Section 2 starts by reviewing the eukaryotic cell cycle
Page 2 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
and DNA repair, and explains one of the proposed models of how cisplatin is believed to achieve
its cytotoxicity, namely that it induces the mismatch repair (MMR) mechanism to enter a futile
cycle of repair, ultimately leading to apoptosis. Section 3 provides an explanation of the known
types of resistance to cisplatin – reduced drug uptake, increased efflux, inactivation by
metallothioneins and glutathione, increased nucleotide excision repair (NER), damage to mismatch
repair mechanisms, homologous recombination and alteration to apoptotic pathways. Section 4
considers the many problems with studying cisplatin resistance : the complex nature of the
signalling pathways involved and the uncertainty as to the exact cytotoxic mechanism may be
masked by the use of non-isogenic cell lines used by different researchers ; the problems of
studying cisplatin resistance in vivo ; the multifactorial nature of cisplatin resistance. Section 5
looks at some ways of overcoming cisplatin resistance – replacing cisplatin itself, developing new
combination therapies, targetting signal transduction pathways, and targetting efflux and
inactivation mechanisms. Several exciting new therapies are being developed in this area, some of
which are just beginning to enter clinical trials. Finally, Section 6 attempts draw some conclusions
about cisplatin resistance and future directions for tackling it.
Figure 1 : Cisplatin
Page 3 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
2 Cancer and Cisplatin
Cancer is a disease of the genes. Over time, changes accumulate in DNA which enhance the
activity of tumour-producing genes (known as proto-oncogenes) and stop the action of tumour-
suppressing genes. DNA damage and errors in DNA replication continue the process leading to
development of a tumour. Chemotherapeutic drugs may be used to target tumour cells and destroy
them by interfering with their ability to grow and divide. Cisplatin is a widely used
chemotherapeutic agent, and cisplatin-based combination therapy is very effective against testicular
cancers, where the cure rate may be up to 95%, but acquired or inherited resistance limits its use in
the treatment of other cancers. In this Section, we start by reviewing the eukaryotic cell cycle and
considering DNA repair mechanisms before looking at how cisplatin is accumulated and how it
achieves its cytotoxic effect.
Figure 2 : Mechanism of action of cisplatin : Cisplatin is taken up from the blood into the cell, singly and/or
doubly aquated and binds as mono- (in the mono-aquated form) or bifunctional adducts. These are believed
to block transcription and/or replication of DNA and ultimately lead to G2 cell cycle arrest and apoptosis.
Page 4 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
2.1 The Eukaryotic Cell Cycle
Figure 3 : The eukaryote cell cycle
The cell cycle of eukaryotes (essentially all organisms whose cells have a nucleus) consists of five
phases. The M phase is the period when cells prepare for and then start the cell cycle. M means
“mitotic”, and this is when the chromosomes are paired and then divided before the cell divides.
The G1 phase is the gap that follows a cell division. Cells here either “decide” to stop dividing and
become terminally differentiated (hence moving in to the G0 phase) or to carry on dividing. One of
the defining characteristics of cancer cells is their inability to stop dividing – they will essentially
never move into G0. The S phase is when DNA is replicated, also known as the DNA synthesis
phase. The G2 phase follows from DNA replication. In this phase, chromosomes start to
condense, nucleoli disappear and the mitotic spindles begin to form from tubulin. It is in this phase
that cisplatin is believed to act. Eukaryotic cells cycle over approximately 16-24 hours when
grown in vitro, but in vivo can vary from 6-8 hours up to 100 days, due to the high variability of the
G1 phase.
Page 5 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
2.2 DNA Repair Mechanisms
DNA is a highly complex molecule whose structure needs constant protection against damage.
Damage recognition proteins are rapidly recruited to areas of DNA damaged or distorted by lesions.
Figure 4 : (a) Types of DNA damaging agent (top), DNA damage (middle) and repair mechanisms (bottom) :
(b) Consequences of DNA damage
These proteins initiate a chain of excision of the adduct and repair of the break thus caused.
Figure 5 shows some of the proteins and complexes involved in the repair of DNA.
Figure 5 : DNA repair proteins : core MMR in dark blue, NER specific in light green, MMR specific in
orange, dual functions are shaded accordingly (eg ERCC-1 is both MMR & NER)
Page 6 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
2.2 DNA Repair Mechanisms (continued)
Tumour cells ”hijack” these genomic integrity maintenance functions and use them to either
increase NER or damage the MMR-protein coding genes. Also, some cisplatin resistant cell lines
are found to express higher levels of particular types of DNA replication proteins (known as
polymerases) which are capable of replicating past cisplatin adducts. Increased NER, which acts to
remove of cisplatin adducts, and defective MMR responses are major causes of cisplatin resistance
- DNA damage repair is often enhanced in all cisplatin resistant cell lines (Marverti 2001).
2.3 Adduct Formation
Cisplatin is administered intravenously. Once it has left the blood where the chloride concentration
is high (~100mM) and entered the cell where the chloride concentration is low (~4mM), its
chloride ligands are aquated (replaced by water molecules). It then forms monofunctional and later
bifunctional cross linked DNA adducts, of which the 1,2-d(GpG) (see Figure 6) intrastrand type
accounts for 65%, also seemingly being most effective cytotoxically (Kartalou & Essigmann
2001a). The other adduct types are 1,2-d(ApG) (25%) and 1,3-d(GpNpG) (5-10%) where N is any
other nucleotide.
Figure 6 : 1,2-d(GpG) adduct
Page 7 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
2.4 Cytotoxicity
Cisplatin is believed to act by blocking DNA replication, leading to cell cycle arrest and ultimately
to apoptosis. One model proposes that cisplatin achieves this by triggering abortive DNA repair
attempts (Kartalou & Essigmann 2001a). These prevent the 1,2-d(GpG) cisplatin adducts from
being effectively repaired, leading to a futile cycle of repair via pathway A (see Figure 7). The
MMR complex of hMSH3/6, hMSH2, hMLH1 and hPMS1/2 is recruited to the adduct, due to the
adduct's bending and unwinding of DNA, where they intitate this futile cycle. This cycle somehow
triggers cell cycle arrest and ultimately apoptosis, which can also be achieved via c-Jun kinase and
c-Abl (pathway B). Neither of these pathways are well understood but are known to be complex.
One study showed 70 proteins up- or downregulated in the cellular injury response to cisplatin
(Johnsson 2001).
Figure 7 : The abortive repair model
Other models propose that : cisplatin hijacks transcription factors such as human upstream binding
factor (hUBF) which is part of the DNA transcription machinery (Treiber 1994); or that it recruits
certain proteins such as HMG1 (Ohndorf 1999) which are believed to block repair of the adducts ;
or that it somehow acts on mitochondria (Dong 1997). None of these models are exclusive.
2.4 Cytotoxicity (continued)
Page 8 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
Cisplatin relies on the excision part of this chain failing and the repair being unable to be executed,
as cisplatin represents the complement to none of the DNA bases. This futile excision/repair cycle
is believed to stall the cell cycle, so that eventually apoptosis is triggered, possibly due to raised
p53 levels.
Page 9 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3 Mechanisms of Cisplatin Resistance
Cisplatin resistance can either be intrinsic or acquired. Intrinsic resistance is the innate ability of
cells to resist treatment, and results from resistance mechanisms which are already present.
Acquired resistance is the result of natural selective pressures operating within the tumour micro-
environment, ensuring that only those cells which are able to survive exposure to fatal levels of
cisplatin will survive. There are many mechanisms of known resistance to cisplatin:
Decreased uptake
Increased efflux
Inactivation by sulfur-containing molecules, such as glutathione
Increased excision of cisplatin adducts
Increased homologous recombination to repair DNA damage
Defects in mismatch repair mechanisms
Increased bypass of cisplatin adducts
Defective apoptotic response or other regulatory protein mutation
Figure 8 : Some mechanisms of resistance to cisplatin
Page 10 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.1 Decreased Uptake
The first step in the formation of cisplatin adducts is for the molecule to enter the cell. As with so
many of the processes involving cisplatin, it is not known exactly how this happens. One study
(Gately 1993) proposes that one-half of cisplatin accumulation takes place via passive diffusion
across the cell membrane while the other half is accounted for via an as yet unknown active pump.
A 48 kilo Dalton (kDa) membrane protein has been found to be expressed in lower levels in
cisplatin resistant cells that show reduced uptake of the drug (Bernal 1990). Another study has
found that ATP is an important requirement for cisplatin uptake in cisplatin sensitive cells but not
in cisplatin resistant cells (Ma 1997). Other studies have shown that certain aldehydes inhibit
cisplatin uptake (Dornish 1986). With these pieces of evidence in mind, one can conjecture a
48kDa protein powered by ATP, which is denatured or inactivated by aldehydes. Also of interest is
the high uptake of cisplatin nanocapsules (cisplatin contained within a lipid coating of around
100nm diameter) recently reported (Burger 2002) (see Figure 9). It is perhaps possible that these
nanocapsules enter the cell by a different mechanism to uncoated cisplatin.
Figure 9 : Cisplatin nanocapsules
(*= cisplatin nanocapsules, MLV= multi lamellar vesicle).
Scale bar 100nm.
Page 11 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.2 Increased Efflux
Some cisplatin.resistant cells have an active method for ridding themselves of cisplatin, a so-called
drug efflux pump. The most well-known drug efflux pumping protein is P-glycoprotein (Pgp), the
product of the mdr gene). This is overexpressed in many multi-drug resistant cells and acts as an
efflux pump. However, cisplatin is not a substrate for Pgp. But some cisplatin resistant cell lines
which display decreased drug accumulation are found to overexpress a 200kDa protein leading to
speculation that this protein may be the efflux pump in the case of cisplatin (Kawai 1990). Another
candidate for the cisplatin drug efflux pump can be found in the MRP family of proteins, which are
related to Pgp – they contain a Pgp-like region (see Figure 10). One member of this family, MRP2,
is often found at high levels in cisplatin-resistant cells (Borst 1999, Schrenk 2001), and others,
MRP3 and MRP5, are often slightly increased (Ishikawa 1992). Confirmation of this comes by
transfecting non-resistant cells with MRP2, which confers resistance to cisplatin (Borst 1999).
Analysis of the differences between the non-cisplatin binding Pgp and MRPx proteins may
highlight the differences between their effects.
Figure 10 : MRP1
The sulphur-rich tripeptide glutathione often binds to cisplatin (see Section 3.3 below), and it is
well known that there exists an efflux pump for glutathione S-conjugates (Ishikawa 1992), and so
cisplatin is also ”ejected” from the cell in this way.
Page 12 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.3 Glutathione and Metallothionein Inactivation
Sulphur-rich molecules such as glutathione (γ-glutamylcysteinyl-glycine, or GSH) and the cysteine-
rich metallothioneins have a high affinity for heavy metals such as platinum and cadmium. It is
believed that, in normal cells, GSH acts to remove reactive species and hence limit DNA damage
(Meister 1983). However, cisplatin resistant cells can also make use of this ability, and it turns out
that GSH and one of GSH’s key enzymes, γ-glutamyltransferase (GGT), have been reported as
often being overexpressed in cisplatin resistant cell lines (Calvert 1998, Daubeuf 2002). The
metallothioneins, like GSH, act to detoxify heavy metals in healthy cells. The evidence
surrounding the rôle of metallothioneins in cisplatin resistance is, however, less clear.
Overexpression of metallothionein has been found in cisplatin resistant cells (Kelley 1988), and
those cell lines which have acquired resistance to cisplatin overexpress metallothionein (Kasahara
1991). Cadmium resistant cell lines overexpressing metallothioneins are also resistant to cisplatin
(Andrews 1987). But curiously it has also been found that transfecting cells with metallothionein
can confer cisplatin sensitivity (Koropatnick 1993).
Page 13 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.4 Increased Nucleotide Excision Repair (NER)
NER is believed to be the main way that adducts are removed from DNA (Ferry 2000) and is a
critical factor in cisplatin resistance. Increased ERCC-1 mRNA levels are found by some studies to
correspond strongly to cisplatin resistance (Li 1999) (see Figure 11). Testicular tumours, which are
highly sensistive to cisplatin, are found to be deficient in the ERCC-1/XPF complex, which could
indicate that it is their inability to repair cisplatin damage which makes them so susceptible.
Figure 11 : (left) Increase over time of messenger RNA (mRNA) levels of a key NER protein, ERCC-1 in a
cisplatin resistant cell line (A2780/CP70) after being continually incubated in the presence of 40 mM of
cisplatin. (right) Concentration response of cisplatin on ERCC-1 mRNA levels in A2780/CP70 by
exposing cells of the line to different concentrations of cisplatin over a 48hr period.
Page 14 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.4 Increased Nucleotide Excision Repair (NER) (continued)
Conversely, some studies have found that deficiency in ERCC-1 renders cells lines more sensitive
to cisplatin (Dunkern 2001) (see Figure 12). The 43-3B cells are deficient in ERCC-1.
Figure 12 : Cell killing in NER deficient cells treated with cisplatin. Survival of CHO-9, 43-3B/ERCC1, 27-1
and 43-3B cells, as determined by colony formation assay, as a function of cisplatin concentration.
However, some authors have reported no correlation between cisplatin response and ERCC-1
mRNA levels (Codegoni 1997). This may be due to the fact that ERCC-1 is most often complexed
with XPF (see Figure 5), and ERCC-1 mRNA levels may not necessarily reflect this (Damia 1998).
Page 15 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.5 Mismatch Repair Mechanisms (MMR)
The cytotoxicity of cisplatin is believed to be strongly dependent upon DNA MMR mechanisms.
Studies have shown that MMR deficient cell lines exhibit high cisplatin resistance. The restoration
of MMR function in these cell lines demonstrably restores cisplatin sensitivity. (Vaisman 1998)
When MMR mechanisms are damaged, the futile cycle of repair which cisplatin depends upon for
its cytotoxicity is broken, and the cell cycle can progress, ensuring that apoptosis is not triggered
and that mutagenicity increases dramatically – one study put the increase at around 3.5 fold. (Lin
1999) Very often cisplatin resistant cell lines are deficient in hMLH1, hMSH2 and/or hMSH6, key
proteins involved in mismatch repair. Interestingly, testicular tumours, which are the tumour type
most successfully treated with cisplatin, express high levels of mismatch repair proteins. (Mello
1996)
Figure 13 : (left) Sensitivity of parental A2780 (♦)cells, MMR deficient cisplatin resistant sublines
A2780/CP70 (□) and A2780/MCP1 (). (right) Restoration of cisplatin sensitivity in A2780/CP79+ch3 ()
with MMR restored vs original cisplatin resistant A2780/CP70 (□).
Page 16 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.6 Increased Adduct Tolerance
DNA is replicated by proteins known as polymerases. DNA polymerase δ/ε normally produce the
leading daughter strand, with polymerase α responsible for producing the lagging strand. However,
when a lesion blocks replication, polymerases ζ-κ come into play specifically to effect translesion
synthesis, along with polymerase β, which can also efficiently replicate past cisplatin adducts. In
the tumour micro-environment, this places a selection pressure on those tumour cells which can
preferentially express polymerases such as DNA polymerase β. Indeed, some ovarian cell cancer
lines overexpress polymerase β by more than 10-fold (Canitrot 2000).
Unfortunately, when an adduct is bypassed, the fidelity of DNA synthesis degrades past the adduct,
as these ”alternative” ploymerases are frequently error prone. This has the unfortunate effect of
introducing mutations into the newly synthesised DNA, which can aid the tumour by providing new
cells with novel chacteristics, some of which may provide still greater resistance potential.
Finally, the tolerance of cisplatin adducts in this way inhibits apoptosis. If the cell no longer cycles
endlessly attempting to effect futile repairs on the adducts, then the regulators of apoptosis, such as
Bax, are downregulated and suppressors of apoptosis such as Bcl-2 are upregulated. In testicular
cancers, some researchers report that Bax is expressed at a high level, and Bcl-2 is expressed at a
low level, further explaining their sensitivity to cisplatin. (Chresta 1996), while others report no
such correlation (Burger 1999).
Page 17 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.7 Homologous Recombination
Homologous recombination (HR) is a mechanism whereby a complementary parent DNA strand
may be used as a template to repair the newly synthesised daughter strand. In Figure 14 (a), the
replication complex is halted (Step 1) by the cisplatin adduct, resulting in a daughter strand gap
(gap between red arrows).
Figure 14 : Daughter strand and double strand gap repair via recombination
Page 18 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.7 Homologous Recombination (continued)
An adduct binding protein (ABP) such as an HMG domain protein may result in a stronger block.
Strand exchange is initiated (Step 2) whereby the original parent strand is used to fill the gap, while
the imperfect synthesised strand (in red) switching to become the complementary strand (Step 3)
and the daughter strand gap is repaired by the original parent strand (Step 4). Finally, the
crossover, known as a Holliday junction, is resolved and the two double stranded DNAs are left,
one with the adduct still attached. In Figure 14 (b), the replication complex collapses due to an
unrepaired gap or nick opposite the adduct. This leaves both a double strand break and a daughter
strand gap. The daughter strand gap is repaired as in (a), while Steps 7-10 ensure the creation of
two intact DNA duplexes (only one is shown). (Zdraveski 2000)
Some studies have shown that cells lines deficient in the initiation of recombination are
hypersensitive to cisplatin, as are those cell lines which are deficient in the resolution of
recombination intermediates. The conclusion is that recombination is as important as NER as a
cellular defense mechanism. (Zdraveski 2000).
Page 19 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
3.8 Regulatory Proteins
The number of proteins found to be up- or downregulated in cellular injury responses (CIR) to
cisplatin is conservatively estimated to be around 70 (Johnsson 2001). The subtle pathways of
inhibition and activation which are driven by the expression of these proteins adds an almost
exponential level of complexity. Figure 15 shows several cellular signalling pathways, including
some, such as the MEK/ERK, Ras, Fos, Myc, c-jun and JNK pathways which are relevant in the
consideration of cisplatin resistance. Some genes have been known to be implicated in cellular
resistance to cisplatin for some time, most notably the oncogenes c-fos, c-myc, c-jun and c-abl and
the tumour suppressor p53. The rôles of others in cisplatin resistance, such as STAT3, IAPs and
V12-Rac1 are just beginning to be made clearer. The proto-oncogene c-fos encodes a nuclear
transcription factor, c-Fos, which induces transcription of a number of genes involved in the
regulation of cell cycle progression, cell replication and differentiation through its interaction with
other proteins. Cisplatin induces expression of c-Fos, which also modulates the expression of genes
which bind the Fos/Jun complex, such as c-myc, metallothionein and polymerase β – all of which
are implicated in cisplatin resistance! (Moorehead and Singh 2000). The oncogene c-myc has been
found in many cisplatin resistant cell lines. The downregulation of c- myc by antisense DNA
restores cisplatin sensitivity. However, as with so much to do with cisplatin resistance, one group
found no correlation between cisplatin resistance and c-myc expression (Osmak 1995). The product
of the gene c-abl is believed to promote cisplatin induced apoptosis. MMR deficient cells fail to
activate c-Abl and seem to be more resistant to cisplatin as a result (Nehme 1997). The activation
of kinase JNK is mediated by c-Abl, and cells which are deficient in c-abl fail to activate JNK in
response to cisplatin damage. Restoration of c-abl in these cells restores JNK activation and
cisplatin sensitivity. Expression of the oncogene c-jun is mediated by JNK.
3.8 Regulatory Proteins (continued)
Page 20 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
C-Jun is overexpressed in cisplatin resistant cells (Zhao 1995). Downregulation of c-jun sensitizes
cells to cisplatin, and leads to reduced expression of DNA repair proteins such as ERCC-1,
although paradoxically cells from c-jun knockout mice are actually more resistant to cisplatin
(Sanchez-Perez 1999). It is believed that the type of cell may play an important part in how c-jun
influences cisplatin resistance.(Leppa 1999). The tumour suppressor gene p53 is involved in the
control of cell cycle, DNA repair and apoptosis, and activates cell cycle arrest at G1 or G2 phases if
DNA damage is present. This gives the cell time to repair the damage. Mutant p53 is a common
feature of cisplatin resistant cell lines, although its complete absence actually sensitises the cell to
cisplatin. (Hawkins 1996). The literature differs quite widely in its conclusions over p53 (Kartalou
& Essigmann 2001b), but the balance of evidence seems to be that mutant p53 cell lines are slightly
more resistant to cisplatin than the wild types (O’Connor 1997). Testicular tumours rarely develop
mutant p53, probably contributing to their susceptibility to cisplatin. STAT3 is a gene involved in
the signal transduction activated by various cytokines and growth factors. It has been found to be
overexpressed in cisplatin-resistant cells (Kato 2000), and is believed to function as an important
mediator of anti-apoptotic signals. Inhibitory of apoptosis proteins (IAPs) are a family of proteins
such as NAIP, c-IAP-2 and survivin which bind with tumour necrosis factor (TNF) factors, thus
blocking apoptotic signals (Notarbartolo 2001). V12-Rac1 is another gene implicated in supressing
apoptosis in the presence of cisplatin by the downregulation of p38, an important kinase involved in
one of the apoptotic pathways (Jeong 2002). Finally, the MEK-ERK “stress” signal transduction
pathway may become suppressed, preventing apoptosis from taking place (Yen Yeh 2002).
Page 21 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
Figure 15 : Signal transduction pathways showing some cisplatin resistance implicated proteins
Page 22 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
4 Problems of Investigating Cisplatin Resistance
Two repeated themes emerge from even a most cursory examinations of the extant research
literature on cisplatin resistance. First is a conclusion which researchers often draw, that cisplatin
resistance is a multifactorial phenomenon. Secondly is the fact that where one group of researchers
has found an effect (say, that protein x induces cisplatin resistance), another group may well find
that protein x either has no impact, or that, perversely, protein x actually induces cisplatin
sensitivity. However, when the details of these studies are examined, it is often the case that the
two groups are not using the same cell lines, indeed, sometimes the cell lines are not even from the
same species. Another aspect of this second issue is the difference between in vivo and in vitro
behaviour of cisplatin and its resistance mechanisms. Most in vitro experiments are performed on
cells cultured in thin layers, whereas, of course, most tumours are solid masses with complex three-
dimensional structures, including blood supplies and interactions and penetrations with supporting
tissues. In vivo experiments on animal models give a more detailed and accurate picture, especially
with murine tumours.
Page 23 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
4.1 Multifactorial Nature of Cisplatin Resistance
Many researchers have noted the multifactorial nature of cisplatin resistance. One group of
researchers tested a number of modulators of cisplatin toxicity in the attempt to reverse cisplatin
resistance (including agents to increase cell permeability, reduce efflux pumping, enhance
accumulation, and inhibt DNA repair) has noted that ”none of the agents tested that modulate
cisplatin sensitivity completely reverse cisplatin resistance. These observations indicate that
multiple mechanisms of resistance arise and more than one may occur in the same cell line when
cells are selected in vitro.” (Akiyama 1999).
Other researchers describe cell lines expressing:
decreased uptake, and MMR defects (Lanzi 1998)
increased inactivation by GSH and GGT, and NER (Daubeuf 2002)
decreased uptake, increased inactivation by GSH and GGT, and NER (Marverti 2001)
decreased uptake, increased inactivation by GSH and GGT, NER and increased
adduct bypass tolerance (Ferry 2000)
etc.
Why is it so often the case that multiple resistance mechanisms are detected? There are two reasons
which I can deduce. Firstly, the mechanisms for protecting the integrity and fidelity of DNA are
highly conserved, and baroque. There are many proteins, and different members of the families of
proteins, which are charged with the transcription, replication and maintenance of DNA. The
signalling pathways within the cell, of which Figure 15 represents but a small part, often exhibit
considerable ”cross talk” – that is, their constituents may influence other, seemingly unrelated,
pathways, and indeed for some reason, overexpression of signalling genes such as c-myc or c-fos
seem to be implicated many different aspects of cisplatin resistance.
Page 24 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
4.1 Multifactorial Nature of Cisplatin Resistance (continued)
Secondly, cell lines such as A2780 exhibit nearly all types of cisplatin resistance, and Ferry et al
stress that ”this is an exaggerated model of resistance, developed by rapidly exposing cells to high
concentrations of cisplatin [and] valuable for for identifying resistance mechanisms and their
underlying molecular basis, but it may not necessarily reflect the underlying clinical drug resistance
phenotype”.
4.2 Cell Lines
Cell lines used in about 20 randomly-selected cisplatin resistance experiments were counted.
Cell Line Studies Origin
C13* (from 2008) 3 Human, ovarian cancer
A2780cisR 2 Human, ovarian cancer
A2780/CP70 2 Human, ovarian cancer
OVCA-429 1 Human, ovarian cancer
OVCA-432 1 Human, ovarian cancer
L1210/DDP 1 Murine, leukemia
A2780CP 1 Human, ovarian cancer
A2780 CP3 1 Human, ovarian cancer
A2780/R 1 Human, ovarian cancer
AOvC-R (from COV413B) 1 Human, ovarian cancer
AOvC-S (from COV413B) 1 Human, ovarian cancer
A2780/C 1 Human, ovarian cancer
SW1573/S1 1 Human, non-small-cell lung cancer
Caco-2 1 Human, colon adenocarcinoma
Tera-CP 1 Human, germ cell
GLC4-CDDP 1 Human, small-cell lung cancer
HeLa-GGT 1 Human, cervical cancer
HeLa-CPR 1 Human, cervical cancer
A431/Pt 1 Human, cervical cancer
TBL.C12 pt 1 Murine, sarcoma
LXFL529 1 Human, non-small-cell lung cancer
CH1cisR 1 Human, ovarian cancer
KFra 1 Human, ovarian cancer
KK 1 Human, ovarian cancer
MH 1 Human, ovarian cancer
SK-OV-3 1 Human, ovarian cancer
Table 1 : Cell lines used in approximately 20 randomly selected cisplatin resistance papers
Page 25 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
4.2 Cell Lines (continued)
Each group of researchers typically took a parental line (for example, CH1 or A2780) and
generated a cisplatin resistant strain by constant exposure to cisplatin. As Ferry et al pointed out,
this procedure produces cell lines which tend to overexpress cisplatin resistance, in a multi-factorial
form, compared to resistant tumours found in vivo. As can be seen from Table 1, very few of the
researchers used the same cell lines, favouring this ”grow it yourself” approach instead. One aspect
not touched on by many researchers is the fact that the cisplatin-resistant cell lines produced in this
way, even if from the same parent cell line, are not isogenic – that is, they are not genetically
identical. That is, if two cultures of parent cell line (say A2780) were used to generate two
cisplatin-resistant cell lines (call them A2780cisA and A2780cisB), there is no guarantee that the
natural selective processes acting on the two parent cell lines would produce identical descendant
cell lines, especially if the culture conditions or length of incubation varied. And so, the types of
cisplatin resistance expressed are likely to be different. The problem is magnified even more when
comparing cell lines from different parents, as there is no possibility of determining to any
precision what selective pressures have been acting upon them in the past. This could in part
explain the conflicting observations between different research groups results when studying
metallothionein (see Section 3.3) and NER (Section 3.4).
Page 26 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
4.3 In Vivo vs In Vitro
To reiterate, in vitro studies of cisplatin resistant cell lines have provided researchers with a
valuable tool for examining cisplatin resistance mechanisms, but the exact extent to which this
knowledge can be ”reverse engineered” into human tumour treatment is unclear. There seems to
be an element to cisplatin-resistant tumours in vivo which is missing in cell culture studies. For
example, cells from a cisplatin resistant murine mammary tumour cultured in monolayers, and
became sensitive to cisplatin. They regained their cisplatin resistance when cultured in three
dimensional multi-cellular tumour spheroids. (Teicher 1990, Kobayashi 1993). Some recent
developments in cell-density dependent processes in tumours, known as quorum sensing, suggest
that gene expression in tumour cells may vary as a function of cell-density, and part of this
signalling system, based around acyl homoserine lactone (AHL) in bacteria, has been found as a
human analogue (Sufrin 2002). It seems highly feasible given the evidence that in addition to the
intracellular processes documented above, a mechanism such as quorum sensing would come into
play with regard to cisplatin resistance at an intercellular level in vivo. The potential for
investigation in this area is considerable.
Page 27 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
5 Prospects for Intervention
There are several strategies for tackling cisplatin resistance including:
replacing cisplatin with a non-cross resistant drug
augmenting cisplatin with drugs or treatments to subdue the resistance mechanisms
other approaches such as novel delivery mechanisms or non-chemical therapies.
Page 28 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
5.1 Replacing Cisplatin
Much effort has been expended on developing platinum complex alternatives to cisplatin. As of
1998, 28 had entered clinical trials, with only four platinum complexes approved for use (cisplatin
and carboplatin globally, oxaliplatin in a few countries and nedaplatin in Japan only), and many
abandoned, although there are many novel platinum compounds at the research stage. Cycloplatam
(ammine cyclopentylamine malato platinum(II) ), being developed in Russia, SKI 2053 (methyl,
isopropyl, dimethylamino, dioxelan malonato platinum(II) ), being developed in Korea, are two
Pt(II) candidates which were in Phase II clinical trials in 1998, and ZD 0473 (cis-amminedichloro
(2-methylpyridine) platinum(II) ), being developed by Astra Zeneca, are three Pt(II) candidates
which were undergoing clinical trials in 1998. JM 216 (bis-acetato-ammine-dichloro-
cyclohexylamine platinum(IV) ) and JM 335 (trans-ammine (cyclohexylaminedichlorodihydroxo)
platinum(IV) ), both being developed by the Johnson-Matthey Company and the Institute of Cancer
Research in the USA, are examples of Pt(IV) complexes being investigated. (Lebwohl & Canetta
1998)
NH3 Cl OH
NH2 Cl
Pt
N Cl Pt
Cl NH3
CH3 OH
Figure 16 : (left) ZD 0473 ; (right) JM335
The commercial stakes are very high. Astra-Zeneca, under pressure, like most of the rest of the
pharmaceutical industry, from rising costs and lengthening drug discovery times, handed out
literature at the 37th American Society of Clinical Oncology meeting in May 2001 describing the
efficacy and safety of ZD 0473 (and other drugs in development) in positive terms. ZD 0473 is a
drug which has not been approved by the FDA for prescription use and as such Astra Zeneca was
issued an FDA warning letter to this effect on 9 July 2001. (FDA 2001)
Page 29 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
5.2 Combination Therapy with Cisplatin
Several drugs work especially well in combination with cisplatin. The most notable are cisplatin
and epotoside (a topisomerase inhibitor, which disrupts the DNA winding and unwinding essential
for transcription and replication), and cisplatin and taxol (an inhibitor of mitosis, which acts to
induce the assembly and stabilisation of microtubules from tubulin – see Section 2.1 for a brief
description of tubulin in the cell cycle).
Pretreatment with buthionine sulfoximine (BSO) acts to reduce GSH levels by inhibiting GGT,
hence possibly reducing the inactivation of cisplatin. (Calvert 1998).
Tirapamazine (TPZ) is a prodrug which, when bioactivated, becomes a highly reactive free radical.
Under hypoxic conditions, TPZ causes single and double strand breaks in DNA. Cells pretreated
with TPZ are more sensitive to cisplatin. (Goldberg 2001).
Pemetrexed disodium is an antifolate which inhibits cancer cell growth. It is currently in Phase III
trials, and has been shown to be particularly active against a broad spectrum of cancers in
combination with cisplatin. (Curtin 2001)
Pretreatment of cisplatin resistant ovarian cancer cells with tamoxifen apparently synergises the
effect of cisplatin. It is proposed that DNA platination is somehow enhanced by the tamoxifen
pretreatment, although this combination has still to enter clinical trials. (Ercoli 1996)
The fluorinated epipodophylloid F 11782, an inhibitor of topoisomerases I and II, has been found
to have a highly synergistic cytotoxic effect when used in combination with cisplatin. It also await
clinical trials. (Barret 2001).
Page 30 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
5.3 Other Approaches
As mentioned in Section 3.1, alternative methods of delivering cisplatin, such as encapsulation in
lipid nanocapsules, improve drug uptake and enhance the cytotoxicty of the drug by up to 1000
fold. (Burger 2002).
The use of hyperthermia (increased heat, 40o C in this case) also improves drug uptake and
enhanced cytoxicity by an unknown mechanism (Ohtsubo 1997).
Electrochemotherapy is the application of high voltage direct current electric pulses to the cells.
This causes the plasma membrane to become more permeable and hence allow enhanced uptake of
drugs such as cisplatin. In a recent murine model study, however, the cure rate was only 6%,
(Cemazar 2001).
Other more speculative approaches include the use of antisense oligonucleotides to block c-fos
(Moorehead and Singh 2000) and c-jun (Pan 2002) expression, and the use of gene therapy to
restore p53 activity, and hence apoptosis (Kanamori 1998).
Page 31 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
6 Conclusion
Cisplatin has been in clinical use now for more than thirty years. In that time it has saved many
lives. Cancer cells, behaving as any species exposed to great natural selective pressures does,
develop resistance as a survival trait over time using the same genomic flexibility which
predisposed them to the cancerous state in the first place. It is clear from what I have read during
the preparation of this review that cisplatin resistance is intimately tied in with the cell cycle and
DNA repair processes that keep cancer cells alive and proliferating. Cisplatin resistance studies to
date are very much the tip of the iceberg, being able to examine only the visible effect of an
enormously complex set of processes. Continued exploration of cellular processes taking into
account the genome, protein folding and binding, biology, chemistry and physics will lead to a
greater understanding of the cell, cancer and cisplatin resistance. Increased understanding of the
tumour environment – how it grows, how it generates new blood supplies – within animals and
humans will also start to fill in the gaps in our knowledge of how cisplatin resistance develops and
is maintained at the macroscopic level. Current treatments in combination with cisplatin have some
considerable effect, but the side effects may be considerable – nausea, vomiting and abdominal
pain. Future treatments will target very specific proteins or receptors and will have very small
effective doses because of this specificity, which will also enable the side effects to be minimised.
It will be interesting to see how the rapidly expanding pool of knowledge about cisplatin’s
mechanism of action and resistance resistance to the drug will affect its use over the next thirty
years, although no doubt cisplatin will go on saving lives for at least as long as that.
Page 32 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
7 Figures & References
Figure 2: From Kartalou & Essigmann 2001a
Figure 3: From Marchesini 2002
Figure 4: From Hoeijmakers 2001
Figure 5 : From Bellacosa 2001
Figure 6 : From Kartalou & Essigman 2001a
Figure 7 : From Kartalou & Essigman 2001a
Figure 8 : From Kartalou & Essigman 2001a
Figure 9 : From Burger 2002
Figure 10 : From Schrenk 2001
Figure 11 : From Li 1999
Figure 12 : From Dunkern 2001
Figure 13 : From Collela
Figure 14 : From Zdraveski 2000
Figure 15 : From Lee & McCubrey 2002
Akiyama S-I, Chen Z-S, Sumizawa T, Furukawa T, Resistance to cisplatin, Anti-cancer Drug
Design 14 (1999) 143-151
Andrews P A, Murphy M P, Howell S B, Metallothionein mediated cisplatin resistance in human
ovarian carcinoma cells, Cancer Chemother. Pharmacol. 19 (1987) 149–154.
Barret J-M et al, Inhibition of nucleotide excision repair and sensitisation of cells to DNA cross-
linking cancer drugs by F11782, a novel fluorinated epipodophylloid, Biochemical Pharmacology
63 (2002) 251-258
Bellacosa A, Functional interactions and signaling properties of mammalian DNA mismatch repair
proteins, Cell Death and Differentiation 8 (2001) 1076-1092
Bernal S D, Speak J A, Boeheim K, Dreyfuss A I, Wright J E, Teicher B A, Rosowksy A, Tsao S
W, Wong Y C, Reduced membrane protein associated with resistance of human squamous
carcinoma cells to methotrexate and cis-platinum, Molecular and Cellular Biochemistry 95 (1)
(1990) 61-70
Borst P, Evers R, Kool M, Wijnholds J, The multidrug resistance protein family, Biochimica et
Biophysica Acta 1461 (1999) 347-357
Burger H, Nooter K, Boersma A W, Kortland C J, Stoter G, Expression of p53, Bcl-2 and Bax in
cisplatin-induced apoptosis in testicular germ cell tumour lines, British Journal of Cancer 77
(1998) 1562-1567
Burger K N J, Staffhorst R W H M, de Vijlder H C, Velinova M J, Boman P H, Frederik P M, de
Kruijff B, Nanocapsules: lipid-coated aggregates of cisplatin with high cytotoxicity, Nature
Medicine 8 (2002) 81-84
Calvert P, Yao K-S, Hamilton T C, O’Dwyer P J, Clinical studies of reversal of drug resistance
based on glutathione, Chemico-Biological Interactions 111-112 (1998) 213-224
Canitrot Y, Hoffmann J S, Calsou P, Hayakawa H, Salles B, Cazaux C, Nucleotide excision repair
DNA synthesis by excess DNA polymerase beta: a potential source of genetic instability in cancer
cells, FASEB J. 14 (2000) 1765-1774
Cemazar M, Miklavcic D, Mir L M, Belehradek Jr, J, Bonnay M, Fourcault D, Sersa
G,Electrochemotherapy of tumours resistant to cisplatin: a study in a murine tumour model,
European Journal of Cancer 37 (2001) 1166–1172
Page 33 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
Chresta C M, Masters J R W, Hickman J A, Hypersensitivity of human testicular tumours to
etoposide-induced apoptosis is associated with functional p53 and a high Bax:Bcl-2 ratio, Cancer
Research 56 (1996) 1834-1841
Codegoni AM, Broggini M, Pitelli M, Torri W, Mangini C, D'Incalci M. Expression of genes of
potential importance in the response to chemotherapy and DNA repair in patients with ovarian
cancer. Gynecol Oncol (1997), 65, 130-137.
Colella G et al, Mismatch repair deficiency is associated with resistance to DNA minor groove
alkylating agents, British Journal of Cancer 80(3/4) (1999), 338-343
Curtin N J, Hughes A N, Pemetrexed disodium, a novel antifolate with multiple targets, The Lancet
Oncology 2 (2001), 298-306
Damia G, Guidi G, D’Incalci M, Expression of genes involved in nucleotide excision repair and
sensitivity to cisplatin and melphalan in human cancer cell lines, European Journal of Cancer 34
(1998) 1783-1788
Daubeuf S, Leroy P, Paolicchi A, Pompella A, Wellman M, Galteau M M, Visvikis A, Enhanced
resistance of HeLa cells to cisplatin by overexpression of γ-glutamyltransferase, Biochemical
Pharmacology 64 (2002) 207-216
Dong Y, Berners-Price S J, Thorburn D R, Antalis T, Dickinson J, Hurst T, Qiu L, Keat Khoo S,
Parsons P G, Serine protease inhibition and mitochondrial dysfunction associated with cisplatin
resistance in human tumour cell lines: targets for therapy, Biochemical Pharmacology 53 (1997)
1673-1682
Dornish J M, Melvik J E, Pettersen E O, Reduced cellular uptake of cis-dichlorodiammine-
platinum by benzaldehyde, Anticancer Res. 6 (1986) 583–588
Dunkern T R, Fritz G, Kaina B, Cisplatin-induced apoptosis in 43-3B and 27-1 cells defective in
nucelotide excision repair, Mutation Research 486 (2001) 249-258
Ercoli A, Scambia G, De Vincenzo R, Alimonti A, Petrucci F, Fattorossi A, Isola G, Benedetti
Panici P, Caroli S, Mancuso S, Tamoxifen synergizes the antiproliferative effect of cisplatin in
human cancer cells; enhancement of DNA platination as a possible mechanism, Cancer Letters 108
(1996) 7-14
FDA warning letter to Astra Zeneca 9 July 2001 http://www.fda.gov/cder/warn/2001/10135.pdf,
accessed 1 October 2002
Ferry K, Hamilton T C, Johnson S W, Increased nulceotide excision repair in cisplatin-resistant
ovarian cancer cells, Biochemical Pharmacology 60 (2000) 1305-1313
Gately D P and Howell S B, Cellular accumulation of the anticancer drug cisplatin: a review,
British Journal of Cancer 67 (1993), 1171-1176
Goldberg Z, Evans J, Birrell G, Brown J M, An investigation of the molecular basis for the
synergistic interaction of tirapazamine and cisplatin, Int. J. Radiation Oncology Biol. Phys., 49(1)
(2001) 175–182
Hawkins D S, Demers G W, Galloway D A, Inactivation of p53 enhances sensitivity to multiple
chemotherapeutic agents, Cancer Research 56 (1996) 892-898
Hoeijmakers J H J, Genome maintenance mechanisms for preventing cancer, Nature 411 (2001)
366-374
Ishikawa T, The ATP-dependent glutathione S-conjugate export pump, Trends Biochem. Sci. 17
(1992) 463–468.
Page 34 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
Jeong H-G, Cho H-J, Chang I-Y, Yoon S-P, Jeon Y-J; Chung M-H, You H J, Rac1 prevents
cisplatin-induced apoptosis through down-regulation of p38 activation in NIH3T3 cells, FEBS
Letters 518 (2002) 129-134
Johnsson A et al, Identification of gene clusters differentially expressed during the cellular injury
responses (CIR) to cisplatin, British Journal of Cancer 85(8) (2001) 1206-1210
Kanamori Y, Kigawa J, Minagawa Y, Irie T, Oishi T, Shimada M, Takahashi M, Nakamura T,
Sato K, Terakawa N, A Newly Developed Adenovirus-mediated Transfer of a Wild-type p53 Gene
Increases Sensitivity to cis-diamminedichloroplatinum (II) in p53-deleted Ovarian Cancer Cells,
European Journal of Cancer 34(11) 1802-1806
Kartalou M, Essigmann JM (2001a), Recognition of cisplatin adducts by cellular proteins,
Mutation Research 478 (2001) 1-21
Kartalou M, Essigmann JM (2001b), Mechanisms of cisplatin resistance, Mutation Research 478
(2001) 23-43
Kasahara K, Fujiwara Y, Nishio K, Ohmori T,.Sugimoto Y, Komiya K, Matsuda T, Saijo N,
Metallothionein content correlates with the sensitivity of human small lung cancer cell lines to
cisplatin, Cancer Res. 51 (1991) 3237–3242.
Kato K, Nomoto M, Izumi H, Ise T, Nakano S, Niho Y, Kohno K, Structure and functional analysis
of the human STAT3 gene promoter: alteration of chromatin structure as a possible mechanism for
the upregulation in cisplatin-resistant cells, Biochimica et Biophysica Acta 1493 (2000) 91-100
Kawai K, Kamatani N, Georges E, Ling V, Identification of a membrane glycoprotein
overexpressed in murine lymphoma sublines resistant to cis-diamminedichloroplatinum(II), J. Biol.
Chem. 265 (1990) 13137–13142.
Kelley S L, Basu A, Teicher B A, Hacker M P, Hamer D H, Lazo J S, Overexpression of
metallothionein confers resistance to anticancer drugs, Science 241 (1988) 1813–1815.
Kobayashi H, Man S, Graham C H, Kapitain S J, Teicher B A, Kerbel R S, Acquired multicellular-
mediated resistance to alkylating agents in cancer, Proc. Nat. Acad. Sci. USA 90 (1993) 3294-3298
Koropatnick J, Pearson J, Altered cisplatin and cadmium resistance and cell survival in Chinese
hamster ovary cells expressing mouse metallothionein, Mol. Pharmacol. 44 (1993) 44–50
Lanzi C, Perego P, Supino R, Romanelli S, Pensa T, Carenini N, Viano I, Colangelo D, Leone R,
Apostoli P, Cassinelli G, Gambetta R A, Zunino F, Decreased Drug Accumulation and Increased
Tolerance to DNA Damage in Tumor Cells with a Low Level of Cisplatin Resistance, Biochemical
Pharmacology 55 (1998) 1247–1254
Lebwohl D, Canetta R, Clinical development of platinum complexes in cancer therapy: an
historical perspective and an update, European Journal of Cancer 34(10) (1998) 1522-1534
Lee J T Jr, McCubrey J A, The Raf/MEK/ERK signal transduction cascade as a target for
chemotherapeutic intervention in leukemia, Leukemia 16 (2002), 486–507
Leppa S, Bohmann D, Diverse functions of JNK signalling and c-Jun in stress response and
apoptosis, Oncogene 18 (1999) 6158-6162
Li Q et al, Modulation of excision repair cross complementation group 1 (ERCC-1) mRNA
expression by pharmacological agents in human ovarian carcinoma cells, Biochemical
Pharmacology 57 (1999) 347-353
Lin X, Kim H-K, Howell S B, The role of DNA mismatch repair in cisplatin mutagenicity, Journal
of Inorganic Biochemistry 77 (1999) 89-93
Page 35 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
Ma J, Maliepaard M, Kolker H J, Verweij J, Schellens J H M, Abrogated energy-dependent uptake
of cisplatin in a cisplatin-resistant subline of the human ovarian cancer cell line IGROV-1, Cancer
Chemotherapy and Pharmacology, 41(3) (1997) 186-192
Marchesini S, Medical Faculty, University of Brescia, Italy,
http://www.med.unibs.it/~marchesi/dna.html accessed 29 September 2002
Maverti G, Bettuzzi S, Astancolle S, Pinna C, Monti M G, Moruzzi M S, Differential indiction of
spermidine/spermine N1-acetyltransferase activity in cisplatin-sensitive and –resistant ovarian
cancer cells in response to N1,N12-bis(ethyl)spermine involves transcriptional and post-
transcriptional regulation, European Journal of Cancer 37 (2001) 281-289
Meister A, Selective modification of glutathione metabolism, Science 220 (1983) 472-477
Mello J A, Acharya S, Fishel R, Essigmann J M, The mismatch repair protein hMSH2 binds
selectively to DNA adducts of the anticancer drug cisplatin, Chem. Biol. 3 (1996) 579-589
Moorehead R A, Singh G, Influence of the proto-oncogene c-fos on cisplatin sensitivity,
Biochemical Pharmacology 59 (2000) 337-345
Nehme A, Baskaran R, Aebi S, Fink D, Nebel S, Cenni B, Wang J Y, Howell S B, Christen R D,
Differential induction of c-Jun NH2-kinase and c-Abl kinase in DNA mismatch repair-proficient
and –deficient cells exposed to cisplatin, Cancer Research 57 (1997) 3253-3257
Notarbartoloa M, Cervellob M, Dusoncheta M, Cusimanoa A, D’Alessandroa N, Resistance to
diverse apoptotic triggers in multidrug resistant HL60 cells and its possible relationship to the
expression of P-glycoprotein, Fas and of the novel anti-apoptosis factors IAP (inhibitory of
apoptosis proteins), Cancer Letters 180 (2002) 91–101
O’Connor P M Jackman J, Bae I, Myers T G, Fan S, Mutoh M, Scudiero D A, Monks A, Sausville
E A, Weinstein J N, Friend S, Fornace A J J, Kohn K W, Characterization of the p53 tumor
suppresor pathway in cell lines of the National Cancer Institute anticancer drug screen and
correlations with the growth-inhibitory potency of 123 anticancer agents, Cancer Research 57
(1997) 4285-4300
Ohndorf U M, Rould M A, He Q, Pabo C O, Lippard S J, Basis for recognition of cisplatin-
modified DNA by high-mobility group proteins, Nature 399 (1999) 708-712
Ohtsubo T, Saito H, Tanaka N, Matsumoto H, Sugimoto C, Saito T, Hayashi S, Kano E,
Enhancement of cisplatin sensitivity and platinum uptake by 40oC hyperthermia in resistant cells,
Cancer Letters 119 (1997) 47-52
Osmak M, Bizjak L, Jernej B, Kapitanovic S, Characterization of carboplatin-resistant sublines
derived from human larynx carcinoma cells, Mutation Research 347 (1995) 141-150
Pan B et al, Reversal of cisplatin resistance in human ovarian cancer cell lines by a c-jun antisense
oligonucleotide (ISIS 10582), Biochemical Pharmacology 63 (2002) 1699-1707
Sanchez-Perez I, Perona R, Lack of c-Jun activity increases survival to cisplatin, FEBS Lett. 453
(1999) 151-158
Schrenk D, Baus P R, Ermel N, Klein C, Vorderstemann B, Kauffmann H-M, Up-regulation of
transporters of the MRP family by drugs and toxins, Toxicology Letters 120 (2001) 51-57
Sufrin J, Roswell Park Cancer Institute, http://www.roswellpark.org/biography_899.html, accessed
1 October 2002
Page 36 of 37 14 oktober 2010
Daen de Leon S807 Mini-Review : Cisplatin Resistance M3852083
Teicher B A, Herman T S, Holden S A, Wany Y, Pfeffer M R, Crawford J W, Frei E III, Tumor
resistance to alkylating agents conferred by mechanisms operative only in vivo, Science 247 (1990)
1457-1461
Treiber D K, Zhai S, Jantzen H M, Essigmann J M, Cisplatin–DNA adducts are molecular decoys
for the ribosomal RNA transcription factor hUBF (human upstream binding factor), Proc. Natl.
Acad. Sci. U.S.A. 91 (1994) 5672–5676
Vaisman A, Varchenko M, Umar A, Kunkel T A, Rissinger J I, Barret J C, Hamilton T C, Chaney
S G, The role of hMLH1, hMSH3 and hMSH6 defects in cisplatin and oxaliplatin resistance:
correlation with replicative bypass of platinum-DNA adducts, Cancer Research 58 (1998) 3579-
3585
Yen Yeh P, Chuang S-E, Yeh K-H, Song Y C, Ea C-K, Cheng A-L, Increase of the resistance of
human carcinoma cells to cisplatin by inhibition of the MEK to ERK signalling pathway partly via
enhancement of anti-cancer drug induced NFκB activation, Biochemical Pharmacology 63 (2002)
1423-1430
Zhao R, Rabo Y B, Egyhazi S, Andersson A, Edgren M R, Linder S, Hansson J, Apoptosis and c-
jun induction by cisplatin in a human melanoma cell line and a drug-resistant daughter cell line,
Anticancer Drugs 6 (1995) 657-668
Zdraveski Z Z, Mello J A, Marinus M G, Essigmann J M, Multiple pathways to recombination
define cellular responses to cisplatin, Chemistry and Biology 7 (2000) 39-50
Thanks to Johanne for her patience and support during the last 8 months – Love Daen
Page 37 of 37 14 oktober 2010
You might also like
- Solid Lipid Nanoparticles: Interaction With Cells, Cytokine Production, and Enzymatic DegradationDocument25 pagesSolid Lipid Nanoparticles: Interaction With Cells, Cytokine Production, and Enzymatic DegradationlithaNo ratings yet
- Long Structured Questions Revision Package 2022Document114 pagesLong Structured Questions Revision Package 2022VincentNo ratings yet
- Midterm 2009 PDFDocument6 pagesMidterm 2009 PDFHyunji KimNo ratings yet
- Cisplatin Resistance and Opportunities For Precision MedicineDocument10 pagesCisplatin Resistance and Opportunities For Precision MedicineRoxanna BallesterosNo ratings yet
- Swan R L 2018Document268 pagesSwan R L 2018Arpan BhattacharyyaNo ratings yet
- Biol 309 Test Question Bank Cell CycleDocument6 pagesBiol 309 Test Question Bank Cell CycleottermanerttwbNo ratings yet
- Biol 309 Test Question Bank Cell CycleDocument6 pagesBiol 309 Test Question Bank Cell CycleMukund VatsNo ratings yet
- Genotoxicity Project 1Document46 pagesGenotoxicity Project 1Vivek DNo ratings yet
- Lippard Mi Tap Latin, A Potent Fusion of Cisplatin and The Orphan Drug DichloroacetateDocument6 pagesLippard Mi Tap Latin, A Potent Fusion of Cisplatin and The Orphan Drug DichloroacetateCezary TomczykNo ratings yet
- Genome Maintenance Meets MechanobiologyDocument22 pagesGenome Maintenance Meets MechanobiologyMARIMORRIS 006No ratings yet
- Nutrigenetica y Nutrigenomica Prevencion Del CancerDocument60 pagesNutrigenetica y Nutrigenomica Prevencion Del CancerSonia LarssonNo ratings yet
- CONFERENCE Abstracts 2021.8.11 UpdatedDocument66 pagesCONFERENCE Abstracts 2021.8.11 UpdatedAnonymous HijNGQtNNo ratings yet
- Cancer Biology - Molecular and Genetic BasisDocument20 pagesCancer Biology - Molecular and Genetic BasisTria KurniawatiNo ratings yet
- Pollutants Cytotoxicity Evaluation Using Allium Cepa Test.Document32 pagesPollutants Cytotoxicity Evaluation Using Allium Cepa Test.ᎯᎻᎷᎬᎠ ᎯshrafNo ratings yet
- FCB Revision Tutorial 2021Document17 pagesFCB Revision Tutorial 2021johnfoxNo ratings yet
- Thiazolidinediones For The Treatment of Type 2 Diabetes EJIM 2007Document8 pagesThiazolidinediones For The Treatment of Type 2 Diabetes EJIM 2007Alexis May UcNo ratings yet
- Choi 1985Document5 pagesChoi 1985FortuneNo ratings yet
- 2015 - The Good and The Bad Faces of STAT1 in Solid TumoursDocument9 pages2015 - The Good and The Bad Faces of STAT1 in Solid TumoursFernando Fernández GarcíaNo ratings yet
- Chemotherapy of Malignancy: Mr.B.CHAKRAPANI M.pharm (PH.D)Document40 pagesChemotherapy of Malignancy: Mr.B.CHAKRAPANI M.pharm (PH.D)besthachakrapaniNo ratings yet
- 先天免疫学糖生物学Document673 pages先天免疫学糖生物学Wenbo Yan100% (1)
- Medical BiochemistryDocument18 pagesMedical BiochemistryKyu Chang HanNo ratings yet
- DNA Repair MechanismssDocument16 pagesDNA Repair MechanismssAqsa AshrafNo ratings yet
- Carcinogenesis and PathogenesisDocument68 pagesCarcinogenesis and PathogenesisSunita KharelNo ratings yet
- Anti Cancer Drugs...Document62 pagesAnti Cancer Drugs...KwirimeNo ratings yet
- The Eukaryotic Cell Cycle and Cancer: in Depth: About This WorksheetDocument8 pagesThe Eukaryotic Cell Cycle and Cancer: in Depth: About This WorksheetddhhdhdhdNo ratings yet
- The Formation of Labyrinths Spots and Stripe Patterns in A Biochemical Approach To Cardiovascular CalcificationDocument16 pagesThe Formation of Labyrinths Spots and Stripe Patterns in A Biochemical Approach To Cardiovascular CalcificationMatteoNo ratings yet
- Campillo NJP 2012Document10 pagesCampillo NJP 2012Pierre NassoyNo ratings yet
- Advanced Drug Delivery Reviews: Ryszard Kole, Arthur M. KriegDocument4 pagesAdvanced Drug Delivery Reviews: Ryszard Kole, Arthur M. KriegInchirah Narimane MgdNo ratings yet
- Cell Cycle and Cell DeathDocument36 pagesCell Cycle and Cell DeathRizky Nur IndahNo ratings yet
- The Physiology and Collective Recalcitrance of Microbial Biofilm CommunitiesDocument54 pagesThe Physiology and Collective Recalcitrance of Microbial Biofilm CommunitiesstartabrezNo ratings yet
- Acfrogasphivh-Xtfhfpduf9lboveax C F2-2hhardm - Fuja64eufnscgzylrzuq6buogp7smhqrx5gxz9es70bkuih2 TJ Ws6cvoavzh 4 Kwdqenvbguq6g5dfpy5ig2ou3yw58utcqdtekDocument3 pagesAcfrogasphivh-Xtfhfpduf9lboveax C F2-2hhardm - Fuja64eufnscgzylrzuq6buogp7smhqrx5gxz9es70bkuih2 TJ Ws6cvoavzh 4 Kwdqenvbguq6g5dfpy5ig2ou3yw58utcqdtekEVEisFunNo ratings yet
- Xie 2001Document17 pagesXie 2001Saheed AbdulkarimNo ratings yet
- Lesson 6Document15 pagesLesson 6DollyNo ratings yet
- Cutin From PlantsDocument12 pagesCutin From Plantsszabolcs_sipos_6No ratings yet
- Iv Fluid Rate Computations: 1. DROPS PER MINUTE (Gtt/min)Document9 pagesIv Fluid Rate Computations: 1. DROPS PER MINUTE (Gtt/min)Luriel BancasoNo ratings yet
- 15 The Cell Cycle-S PDFDocument6 pages15 The Cell Cycle-S PDFAml Aml0% (1)
- Regulation of Cell Division: DR Sri WidyartiDocument49 pagesRegulation of Cell Division: DR Sri WidyartiMaheer JoefrieNo ratings yet
- Adherens and Tight Junctions: Structure, Function and Connections To The Actin CytoskeletonDocument10 pagesAdherens and Tight Junctions: Structure, Function and Connections To The Actin Cytoskeletonanirbanmanna88320No ratings yet
- Cell Cycle & Its RegulationDocument16 pagesCell Cycle & Its RegulationElina GNo ratings yet
- 0-DISERTACIJA AkramieneDocument90 pages0-DISERTACIJA AkramieneHimanshu PanchalNo ratings yet
- Week7 ExplorationHomeworkDocument3 pagesWeek7 ExplorationHomeworkShannon KelsoNo ratings yet
- Moe Et Al-2015-Seminars in Cell & Developmental BiologyDocument6 pagesMoe Et Al-2015-Seminars in Cell & Developmental BiologyMichael DaleyNo ratings yet
- Cellcycle Worksheet PDFDocument7 pagesCellcycle Worksheet PDF2022: Moises AkermanNo ratings yet
- Colorectal Cancer Cell Lines Show Striking Diversity of Their O-Glycome Reflecting The Cellular Differentiation PhenotypeDocument14 pagesColorectal Cancer Cell Lines Show Striking Diversity of Their O-Glycome Reflecting The Cellular Differentiation PhenotypeRapazito RagazzoNo ratings yet
- Ch. 13-Cytoskeletal SystemsDocument18 pagesCh. 13-Cytoskeletal Systemsnkorkmaz1357No ratings yet
- Cell Biology: The Cell Division CylceDocument56 pagesCell Biology: The Cell Division Cylcebabybri94No ratings yet
- Unit 1Document52 pagesUnit 1Dsce BtNo ratings yet
- 1 s2.0 S1348864311000073 MainDocument5 pages1 s2.0 S1348864311000073 MainSuleiman DaudaNo ratings yet
- Document 3Document16 pagesDocument 3Citra AuraNo ratings yet
- Cell DivisionDocument40 pagesCell DivisionMohamed NourNo ratings yet
- Huntington CureDocument12 pagesHuntington CureJuan Pablo PérezNo ratings yet
- Biology 212: Cell Biology Final ExamDocument7 pagesBiology 212: Cell Biology Final ExamtimNo ratings yet
- Qa 6Document2 pagesQa 6Debapriya HazraNo ratings yet
- Metaphase: Genome Mitosis Mitotic SpindleDocument2 pagesMetaphase: Genome Mitosis Mitotic SpindleYut3No ratings yet
- Chapter+2Cell+Proliferation Onco CeliaDocument34 pagesChapter+2Cell+Proliferation Onco CeliaPaula C GuimaraesNo ratings yet
- How Cisplatin Works On Treating CancerDocument2 pagesHow Cisplatin Works On Treating CancermeimeiliuNo ratings yet
- Role of Cholesterol in The Function and Organization of G-Protein Coupled Receptors (Pucadyil and Chattopadhyay, 2006)Document39 pagesRole of Cholesterol in The Function and Organization of G-Protein Coupled Receptors (Pucadyil and Chattopadhyay, 2006)Leo TolentinoNo ratings yet
- Membrane Lipid Signaling in Aging and Age-Related DiseaseFrom EverandMembrane Lipid Signaling in Aging and Age-Related DiseaseNo ratings yet
- Kami Export - Maxwell Modeste - Photosynthesis Case Study - Killing ChloroplastsDocument7 pagesKami Export - Maxwell Modeste - Photosynthesis Case Study - Killing ChloroplastsMaxwell Modeste0% (2)
- Integration of Metabolism WebDocument72 pagesIntegration of Metabolism WebLini Anisfatus SholihahNo ratings yet
- DNA: Structure & FunctionDocument3 pagesDNA: Structure & Function孙美美Ezra Paola TaysonNo ratings yet
- NSEJS-CAMP Assignment - Plant PhysiologyDocument3 pagesNSEJS-CAMP Assignment - Plant PhysiologyetrdrssNo ratings yet
- Bacterial Quantification MCQsDocument3 pagesBacterial Quantification MCQsMahi ShafiqueNo ratings yet
- Chapter 3 Material 3) Inevitability of ErrorDocument26 pagesChapter 3 Material 3) Inevitability of ErrorJilly CookeNo ratings yet
- CELL CYCLE McqsDocument2 pagesCELL CYCLE McqsHamzullah KhanNo ratings yet
- 11 OperonDocument24 pages11 OperonSanghaviNo ratings yet
- EXAM - Introductory Biochemistry and Molecular Biology (Jan 2016) PDFDocument9 pagesEXAM - Introductory Biochemistry and Molecular Biology (Jan 2016) PDFcatalinauroraNo ratings yet
- McKee Chapter8 Sample PDFDocument44 pagesMcKee Chapter8 Sample PDFMustafa Kırca100% (1)
- Unacademy 1Document18 pagesUnacademy 1ANUPAM ANAND KUMAR PANDEY MBA-INo ratings yet
- Bioenergetics HandoutDocument1 pageBioenergetics HandoutRhaven GonzalesNo ratings yet
- Stages of Mitosis Lab ReportDocument3 pagesStages of Mitosis Lab ReportNor Ashikin Ismail67% (6)
- Ijms 19 00311Document26 pagesIjms 19 00311Hidayat ArifinNo ratings yet
- Genetic Codes With No Dedicated Stop Codon Context Dependent Translation TerminationDocument13 pagesGenetic Codes With No Dedicated Stop Codon Context Dependent Translation TerminationAarcamNo ratings yet
- Chemistry of CarbohydratesDocument10 pagesChemistry of CarbohydratesYahya Daham Zafeer SakhrNo ratings yet
- The Identification of OncogenesDocument43 pagesThe Identification of OncogenesRicha PandeyNo ratings yet
- #U0633#U0643#U0646#U062 FDocument30 pages#U0633#U0643#U0646#U062 Frahaf hussienNo ratings yet
- Las Q4 Week-2 GenDocument8 pagesLas Q4 Week-2 GenFranzhean Balais CuachonNo ratings yet
- Mitosis - WikipediaDocument39 pagesMitosis - WikipediaMuhammad Azhar MagsiNo ratings yet
- pCDFDuet-1 Map PDFDocument2 pagespCDFDuet-1 Map PDFesn_kNo ratings yet
- Lipid Metabolism MCQs (Cholesterol, Triglycerides, and Other Lipids) - 1639455481990Document8 pagesLipid Metabolism MCQs (Cholesterol, Triglycerides, and Other Lipids) - 1639455481990Lola MuhozaNo ratings yet
- Topik 3 Cell Division PAST YEAR QUESTIONSDocument9 pagesTopik 3 Cell Division PAST YEAR QUESTIONSIslahNo ratings yet
- Cancer and The Cell CycleDocument42 pagesCancer and The Cell CycleBrayan CuevasNo ratings yet
- Chemistry of Signals and ReceptorsDocument13 pagesChemistry of Signals and Receptorsour lectureNo ratings yet
- Gluconeogenesis: The Pathway and RegulationDocument31 pagesGluconeogenesis: The Pathway and RegulationMunachande KanondoNo ratings yet
- Training Energy Systems Through IntervalsDocument19 pagesTraining Energy Systems Through IntervalsIndu G MathiNo ratings yet
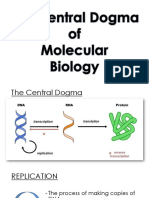
- 3.7 Central DogmaDocument28 pages3.7 Central DogmaJovit Angelo David100% (1)
- Budget-of-Work-General Biology 1Document2 pagesBudget-of-Work-General Biology 1joei ArqueroNo ratings yet
- DNA Translation J Muqaddas MukhtarDocument33 pagesDNA Translation J Muqaddas MukhtarSafia DurraniNo ratings yet