You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- DOH Test Results Info FINALDocument1 pageDOH Test Results Info FINAL10News WTSPNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Strategic Management of Health Care Organizations 8th Edition Ginter Duncan Swayne Test BankDocument12 pagesThe Strategic Management of Health Care Organizations 8th Edition Ginter Duncan Swayne Test BankYasmine Abdelbary100% (2)
- Role of Community Case ManagerDocument11 pagesRole of Community Case ManagerHo PingNo ratings yet
- Letter To Toronto Medical Officer of HealthDocument2 pagesLetter To Toronto Medical Officer of HealthCityNewsToronto50% (4)
- Accreditation BookDocument522 pagesAccreditation BookBungKee Iscmu100% (4)
- Resonance of A Closed Air ColumnDocument11 pagesResonance of A Closed Air ColumnHo Ping100% (6)
- Ethical DilemmaDocument6 pagesEthical DilemmaHo PingNo ratings yet
- Hyperemesis GravidarumDocument17 pagesHyperemesis GravidarumHo PingNo ratings yet
- Causes of The Formation of Nurse Midwifery in The United States During The Early Twentieth CenturyDocument16 pagesCauses of The Formation of Nurse Midwifery in The United States During The Early Twentieth CenturyHo PingNo ratings yet
- Wong-Baker Faces ScaleDocument10 pagesWong-Baker Faces ScaleHo Ping100% (1)
- Social, Philosophical, and Economic Causes of The French RevolutionDocument19 pagesSocial, Philosophical, and Economic Causes of The French RevolutionHo Ping67% (3)
- Legal and EthicalDocument9 pagesLegal and EthicalHo PingNo ratings yet
- Key Performance Indicators (Kpi) For The Medical Officer (Reg/Con) (Name DR B Suresh Babu) of PHC Parumanchala For The Month ofDocument2 pagesKey Performance Indicators (Kpi) For The Medical Officer (Reg/Con) (Name DR B Suresh Babu) of PHC Parumanchala For The Month ofZEETECH COMPUTERSNo ratings yet
- 5831Document45 pages5831rahimulNo ratings yet
- Violence Against Women PDFDocument91 pagesViolence Against Women PDFFairyNo ratings yet
- dm2022 0304Document2 pagesdm2022 0304Charlemagne Sabio GalamgamNo ratings yet
- Purpose of BABE: Chu Yuan ShanDocument9 pagesPurpose of BABE: Chu Yuan ShanJessie ChuNo ratings yet
- Clinical Practice Guideline For An Infection Controlexposure Control Program in The Oral Healthcare SettingDocument1 pageClinical Practice Guideline For An Infection Controlexposure Control Program in The Oral Healthcare Settingapi-399847495No ratings yet
- Leave Application FormDocument2 pagesLeave Application FormRPh Krishna Chandra Jagrit50% (2)
- Professional Growth and Development: University of Southern MindanaoDocument70 pagesProfessional Growth and Development: University of Southern MindanaoAYOB, Baiwata B.No ratings yet
- Global Health Security From The World Health OrganizationDocument12 pagesGlobal Health Security From The World Health OrganizationRainer A.No ratings yet
- QAS Process Overview Cairo - 082018Document45 pagesQAS Process Overview Cairo - 082018KaRiM NassarNo ratings yet
- Health Care Policy and Delivery Systems SyllabusDocument6 pagesHealth Care Policy and Delivery Systems SyllabusDeekay100% (1)
- 7AN01TE0220 Part 1 CorrectionDocument9 pages7AN01TE0220 Part 1 CorrectionOrnella ANAGONOU-ZODJINo ratings yet
- Sample CBDRP Activity DesignDocument9 pagesSample CBDRP Activity DesignJa NiceNo ratings yet
- Where Should I Inject VaccinesDocument1 pageWhere Should I Inject VaccinesJaneNo ratings yet
- Poison Schedule SummaryDocument1 pagePoison Schedule SummaryHenriettaNo ratings yet
- Effect of Chest PackDocument2 pagesEffect of Chest PacksureshbabubnysNo ratings yet
- ფიზიოლოგიური მშობიარობის მართვაDocument30 pagesფიზიოლოგიური მშობიარობის მართვაAchi BeridzeNo ratings yet
- Lesson 2Document2 pagesLesson 2Ma. Brittany Stacy Le BerongoyNo ratings yet
- Army Manage Vaccination Centres - 31 Aug 2021Document1 pageArmy Manage Vaccination Centres - 31 Aug 2021poornimaNo ratings yet
- The Efficacy of International Health Regulations in Pandemic Response and Management Essay PlanDocument4 pagesThe Efficacy of International Health Regulations in Pandemic Response and Management Essay PlankymhanNo ratings yet
- Ibd Makalah Kel.2Document1 pageIbd Makalah Kel.2Haura AlbaninaNo ratings yet
- Training Manual For State & District Surveillance Officers: Integrated Disease Surveillance ProjectDocument12 pagesTraining Manual For State & District Surveillance Officers: Integrated Disease Surveillance ProjectHosam GomaaNo ratings yet
- Materi UTS Global HealthDocument141 pagesMateri UTS Global HealthNurul AnggrainiNo ratings yet
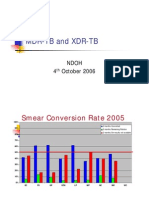
- MDR-TB and XDR-TB: Ndoh 4 October 2006Document40 pagesMDR-TB and XDR-TB: Ndoh 4 October 2006Eta Calvin ObenNo ratings yet
- NafisaDocument8 pagesNafisasry yanaNo ratings yet
- Safe Motherhood Ordinance 2011Document17 pagesSafe Motherhood Ordinance 2011Dhonnalyn Amene Caballero100% (1)