You might also like
- 4 - Anatomy and Kinesiology of The ShoulderDocument8 pages4 - Anatomy and Kinesiology of The ShoulderLeanna NNo ratings yet
- Luxacion de HombroDocument25 pagesLuxacion de HombroAlex ChavezNo ratings yet
- Shoulder Anatomy & Biomechanics (Halder) PDFDocument18 pagesShoulder Anatomy & Biomechanics (Halder) PDFNedelcuGeorgeNo ratings yet
- Rotator Cuff Injuries and Their Management (20-01-22)Document76 pagesRotator Cuff Injuries and Their Management (20-01-22)aishp2897No ratings yet
- Ould R: Applied AnatomyDocument4 pagesOuld R: Applied Anatomyayu feratywiNo ratings yet
- Shoulder Biomechanics: Roberto Lugo, Peter Kung, C. Benjamin MaDocument11 pagesShoulder Biomechanics: Roberto Lugo, Peter Kung, C. Benjamin MaAbyudya Rafif KurniawanNo ratings yet
- Opa 220-230Document11 pagesOpa 220-230Hijrana PutriNo ratings yet
- Biomechanics Rotator CuffDocument8 pagesBiomechanics Rotator CuffVivian KeungNo ratings yet
- Polkowski 2010Document7 pagesPolkowski 2010chan kyoNo ratings yet
- Glenohumeral Joint Instability: ReviewDocument15 pagesGlenohumeral Joint Instability: ReviewOrto MespNo ratings yet
- Elbow Anatomy & Biomechanics (Fornalski,)Document11 pagesElbow Anatomy & Biomechanics (Fornalski,)Gloria Pg MontzeNo ratings yet
- Dynamic Stability of The Glenohumeral JointDocument16 pagesDynamic Stability of The Glenohumeral JointFranco RojasNo ratings yet
- Reverse ShoulderreplacementDocument8 pagesReverse ShoulderreplacementagniosaiNo ratings yet
- Shoulder Arthroplasty WIC - Dr. LSDocument56 pagesShoulder Arthroplasty WIC - Dr. LSDifitasari Cipta Perdana100% (1)
- Stryker Shoulder ArthroplastyDocument10 pagesStryker Shoulder Arthroplastymuhammad umarNo ratings yet
- Anatomy and Bio Mechanics of The KneeDocument15 pagesAnatomy and Bio Mechanics of The KneeaimanshalpyNo ratings yet
- BiomechanicDocument15 pagesBiomechanicMuhamad SdeqNo ratings yet
- Ould R: Applied AnatomyDocument6 pagesOuld R: Applied Anatomyayu feratywiNo ratings yet
- Finnoff Glenohumeral Instdsability and Dislocation PDFDocument31 pagesFinnoff Glenohumeral Instdsability and Dislocation PDFSoriana MureşanNo ratings yet
- Anterior Shoulder InstabilityDocument19 pagesAnterior Shoulder InstabilitySiti Nur JannahNo ratings yet
- Magee HombroDocument130 pagesMagee HombroJorge Vargas CatalanNo ratings yet
- Glenohumeral JointDocument85 pagesGlenohumeral JointPoojitha reddy MunnangiNo ratings yet
- At 0624Document6 pagesAt 0624DanDezideriuIacobNo ratings yet
- Condition Chart Shoulder ImpingementDocument18 pagesCondition Chart Shoulder Impingementapi-547889945No ratings yet
- Rotator Cuff Biology and Biomechanics: A Review of Normal and Pathological ConditionsDocument9 pagesRotator Cuff Biology and Biomechanics: A Review of Normal and Pathological ConditionsmatteoNo ratings yet
- Rotator Cuff Biology and Biomechanics: A Review of Normal and Pathological ConditionsDocument9 pagesRotator Cuff Biology and Biomechanics: A Review of Normal and Pathological ConditionsmatteoNo ratings yet
- ShoulderinestabDocument16 pagesShoulderinestabIsidora SchalschaNo ratings yet
- Kibler 2016 The Role of The Scapula in Preventing and Treating Shoulder Instability PDFDocument8 pagesKibler 2016 The Role of The Scapula in Preventing and Treating Shoulder Instability PDFPamela DíazNo ratings yet
- V67N1 4 PDFDocument8 pagesV67N1 4 PDFAndrésOlivaRossiNo ratings yet
- Anterior Shoulder Instability A Review of PathoanatomyDocument8 pagesAnterior Shoulder Instability A Review of PathoanatomyNikita TripthiNo ratings yet
- Centric RelationDocument18 pagesCentric RelationKrupali JainNo ratings yet
- Recurrent Dislocation of The ShoulderDocument31 pagesRecurrent Dislocation of The ShoulderDiana AstriaNo ratings yet
- Physical Therapy For The Treatment of Shoulder InstabilityDocument16 pagesPhysical Therapy For The Treatment of Shoulder InstabilityDelaram IravaniNo ratings yet
- Biomechanics of The Shoulder: Dennis L. Hart, Mpa, PT, Stephen W. Carmichael, PHDTDocument6 pagesBiomechanics of The Shoulder: Dennis L. Hart, Mpa, PT, Stephen W. Carmichael, PHDTPrem KumarNo ratings yet
- Scapular Dyskinesia, The Forgotten Culprit of Shoulder Pain and How To RehabilitateDocument6 pagesScapular Dyskinesia, The Forgotten Culprit of Shoulder Pain and How To RehabilitateQuiroprácticaParaTodosNo ratings yet
- Biomechanics of Elbow ComplexDocument9 pagesBiomechanics of Elbow ComplexKIARA VENICE DELGADONo ratings yet
- Functional Anatomy ShoulderDocument8 pagesFunctional Anatomy ShoulderJohannesSchoppmannNo ratings yet
- (2011) Hip InstabilityDocument19 pages(2011) Hip InstabilityRouss Sepúlveda CastilloNo ratings yet
- Rehabilitation of Shoulder Impingement Syndrome and Rotator Cuff Injuries: An Evidence-Based ReviewDocument10 pagesRehabilitation of Shoulder Impingement Syndrome and Rotator Cuff Injuries: An Evidence-Based ReviewEduardo Santana SuárezNo ratings yet
- Shoulder Kines (Autosaved)Document86 pagesShoulder Kines (Autosaved)niekoNo ratings yet
- 03 - Clinical Bio Mechanics of The Oral JointDocument7 pages03 - Clinical Bio Mechanics of The Oral JointaimanshalpyNo ratings yet
- Current Concepts of Posterolateral Corner Injuries of The Knee 2017Document13 pagesCurrent Concepts of Posterolateral Corner Injuries of The Knee 2017Mohan DesaiNo ratings yet
- 2017 OITE ReviewDocument105 pages2017 OITE ReviewJayNo ratings yet
- Anterior Shoulder DislocationDocument121 pagesAnterior Shoulder DislocationAnupama SNo ratings yet
- Centric Relation: Controversies Surrounding It: Centric Relation Has No Function - A Realistic SuppositionDocument22 pagesCentric Relation: Controversies Surrounding It: Centric Relation Has No Function - A Realistic SuppositionNikita AggarwalNo ratings yet
- TKA Total Knee ARTHROPLASTY Replacement Conf 2Document96 pagesTKA Total Knee ARTHROPLASTY Replacement Conf 2haminatrafNo ratings yet
- Anatomy of The Elbow: Trauma and ReconstructionDocument13 pagesAnatomy of The Elbow: Trauma and ReconstructionSrinivasNo ratings yet
- Complex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDDocument14 pagesComplex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDAndrea Z MilanoNo ratings yet
- Biomechanical Factors in Rotator Cuff PathologyDocument5 pagesBiomechanical Factors in Rotator Cuff PathologyYa ChenNo ratings yet
- William C. Cottrell, MD AbstractDocument4 pagesWilliam C. Cottrell, MD AbstractmalaNo ratings yet
- Lecture 3 Elbow ComplexDocument24 pagesLecture 3 Elbow ComplexIbraheem MohdNo ratings yet
- Glenoid LabrumDocument26 pagesGlenoid LabrumluizamgoNo ratings yet
- Hombro Artroscopia 1.2Document15 pagesHombro Artroscopia 1.2lyneth lacourtNo ratings yet
- 1-Prof DR Anees Biomechanics of HipDocument63 pages1-Prof DR Anees Biomechanics of HipAhmed M3tmdNo ratings yet
- Labrum PosteriorDocument13 pagesLabrum PosteriorMustika Ainun FadhilaNo ratings yet
- Evaluacion Inestabilidad HombroDocument13 pagesEvaluacion Inestabilidad HombroIvan ReyesNo ratings yet
- Alingment in TKRDocument3 pagesAlingment in TKRdeepak100% (1)
- Floating Shoulder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFloating Shoulder, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Re-Integrate Patterns of Overwhelm, Trauma and Emotional HoldingDocument2 pagesRe-Integrate Patterns of Overwhelm, Trauma and Emotional HoldingIsabel ValdésNo ratings yet
- How To Lucid Dream Peach BlackDocument4 pagesHow To Lucid Dream Peach BlackIsabel ValdésNo ratings yet
- Induction of Lucid Dreams: A Systematic Review of Evidence: Author NoteDocument57 pagesInduction of Lucid Dreams: A Systematic Review of Evidence: Author NoteIsabel ValdésNo ratings yet
- Cognitive and PsychologicalDocument23 pagesCognitive and PsychologicalIsabel ValdésNo ratings yet
- Neural Correlates of Virtual Route Recognition in Congenital BlindnessDocument6 pagesNeural Correlates of Virtual Route Recognition in Congenital BlindnessIsabel ValdésNo ratings yet
- Soothe Your Sciatica: SolutionsDocument7 pagesSoothe Your Sciatica: Solutionsanand sahuNo ratings yet
- 15-Van Oostveen Et AlDocument11 pages15-Van Oostveen Et AlBenedictus Anindita SatmokoNo ratings yet
- DLL - Science 6 - Q2 - W1Document5 pagesDLL - Science 6 - Q2 - W1Janette EvangelistaNo ratings yet
- Lower LimbDocument9 pagesLower LimbCrishu Razvi100% (4)
- Bobath ApproachDocument22 pagesBobath ApproachCedricFernandez50% (4)
- Spinal Cord InjuryDocument27 pagesSpinal Cord InjuryHanis Malek100% (1)
- Screenshot 2023-01-10 at 11.40.36 AMDocument67 pagesScreenshot 2023-01-10 at 11.40.36 AMAnchal LohanaNo ratings yet
- Prosthetics and Orthotics Manufacturing Guidelines: Lower Limb Orthotics: Ankle-Foot OrthosisDocument31 pagesProsthetics and Orthotics Manufacturing Guidelines: Lower Limb Orthotics: Ankle-Foot OrthosisInternational Committee of the Red Cross100% (1)
- The Better Movement BlueprintDocument26 pagesThe Better Movement BlueprintTim LaneNo ratings yet
- The Influence of Altered Lower-Extremity Kinematics On Patellofemoral Joint Dysfunction - Powers 2003Document8 pagesThe Influence of Altered Lower-Extremity Kinematics On Patellofemoral Joint Dysfunction - Powers 2003shivnairNo ratings yet
- Closed Fractures of The Tibial Diaphysis: David L. Rothberg, MD Erik N. Kubiak, MDDocument64 pagesClosed Fractures of The Tibial Diaphysis: David L. Rothberg, MD Erik N. Kubiak, MDtilahunthmNo ratings yet
- Anatomy and Surgical Appraches of The Temporal Bone PDFDocument251 pagesAnatomy and Surgical Appraches of The Temporal Bone PDFMihai Mitza100% (5)
- Epidemiology of Knee Injuries Diagnosis and TriageDocument3 pagesEpidemiology of Knee Injuries Diagnosis and TriageRuben CapelaNo ratings yet
- Jaspal R Singh, M.D.: Department of Rehabilitation MedicineDocument2 pagesJaspal R Singh, M.D.: Department of Rehabilitation MedicineshikhaNo ratings yet
- Lean Muscle ProgramDocument2 pagesLean Muscle ProgramtonypodmoreNo ratings yet
- The Association Between Lumbar Rib and Lumbosacral Transitional VertebraeDocument14 pagesThe Association Between Lumbar Rib and Lumbosacral Transitional VertebraeAnGBalNo ratings yet
- ACL GuideDocument5 pagesACL GuideEvans JohnNo ratings yet
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Document6 pagesSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangoneNo ratings yet
- The Difficult Knee Severe Varus and Valgus.6Document6 pagesThe Difficult Knee Severe Varus and Valgus.6Louie OkayNo ratings yet
- LES MILLS CORE 53 (CORE53ChoreographyNotes Row en App Print PDFDocument40 pagesLES MILLS CORE 53 (CORE53ChoreographyNotes Row en App Print PDFchris.hutton9898No ratings yet
- Subtrochanteric Femur Fractures: Asheesh Bedi, MD, T. Toan Le, MDDocument11 pagesSubtrochanteric Femur Fractures: Asheesh Bedi, MD, T. Toan Le, MDMd.Shafiul EzazNo ratings yet
- Burrows and Moreton Prize0Document4 pagesBurrows and Moreton Prize03nhu1100% (1)
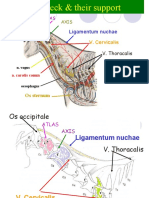
- Hanakep 2 Neck SC Ii 2020Document47 pagesHanakep 2 Neck SC Ii 2020Hana AdivaNo ratings yet
- Rehabilitation Procedures For A Hamstring TearDocument2 pagesRehabilitation Procedures For A Hamstring TearB W100% (1)
- Ligamentos de La ManoDocument9 pagesLigamentos de La ManoEnrique Maturana SepulvedaNo ratings yet
- Body MechanicsDocument7 pagesBody MechanicsKristine CustodioNo ratings yet
- Therapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.13Document30 pagesTherapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.13Mustafa ,GhulamNo ratings yet
- Clinical Upper Limb OsmosisDocument11 pagesClinical Upper Limb OsmosisAdirfah AmeriyaniNo ratings yet
- Muscular System MindmapDocument1 pageMuscular System MindmapMayeliz UrvinaNo ratings yet
- Science Time Bones Lesson PlanDocument52 pagesScience Time Bones Lesson Planapi-547839068No ratings yet