NURSING CARE PLAN
Patient’s Name: Palon, Eduardo Name: Jesse James Edjec
Age: Group 2 BN3-N
Sex: M
Marital Status:
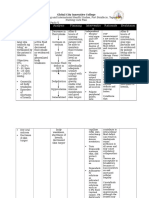
CC: loose watery stool
Medical Diagnosis: Acute gastroenteritis with moderate dehydration
Date of Admission: May 5, 2010
Time of Admission:
Assessment Data Nursing Rationale Desired Outcome Nursing Interventions Justification Evaluation
Diagnosis
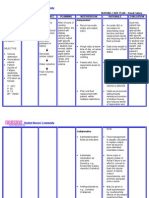
Increase Output After 16hours of nurse-client
Independent intervention, the client was
Actual/Abnormal Fluid Volume (diarrhea) At the end of 16hrs nurse- able to:
Findings deficit related to client intervention, the client
loose watery Decrease in total will be able to: 1. Assess vital signs; note strength of -To evaluate degree of fluid
peripheral pulses. deficit.
Subjective: stool (Diarrhea) body water
• Thirst AEB thirst, 1. Maintain fluid volume at a 2. Keep fluids within clients reach -to correct/ replace losses to
• Weakness weakness, reductions in both the functional level as evidenced and encourage frequent intake as reverse pathophysiologic
Objective: decreased urine intracellular and by individually adequate appropriate. mechanisms.
• Decreased urine output, poor skin extracellular fluid urinary output with normal
output turgor, BP- volumes specific gravity, stable vital 3. Control humidity and ambient air -To reduce high fever and
100/80, Pulse-84 signs, moist mucous temperature as appropriate. Reduce elevated metabolic rate.
• Poor skin turgor membranes, good skin turgor beddings/clothes, provide tepid
intravascular volume
• BP-100-80 Definition: depletion and prompt capillary refill. sponge bath.
• Pulse-84 Decreased
Risk Related Factors 4. Change position frequently. -To promote comfort and
intravascular, thirst, weakness, 2. Verbalize understanding of
• Anxiety safety.
interstitial, decreased urine output, causative factors and purpose
• Infrequent fluid and/or poor skin turgor, of individual therapeutic 5. Provide safety measures when -To promote safety.
intake intracellular decrease BP, increase interventions and medications. client is confused.
Strengths fluid. This refers pulse rate and
• Strong family to dehydration, temperature 3. Demonstrate behaviors to Collaborative -to limit gastric/intestinal
support water loss alone monitor and correct deficit as 1. Administer medications as losses.
indicated.(antidiarrheals)
• Strong without sodium. Fluid Volume Deficit indicated.
Compliance to 2. Establish 24-hour fluid -To prevent peaks/valleys in
medications Definition: Reference: replacement needs and fluid level.
Reference: http://emedicine.me routes to be used.
Nurse’s pocket dscape.com/article/
Guide 9th edition 906999-overview 3. Administer IV fluids as -To replace losses to reverse
indicated. pathophysiologic
mechanisms.
You might also like
- Deficient Fluid Volume (AGEDocument2 pagesDeficient Fluid Volume (AGENursesLabs.com83% (6)
- NCP - AgeDocument5 pagesNCP - Ageunsp3akabl386% (7)
- NCP Risk For Fluid Volume DeficitDocument2 pagesNCP Risk For Fluid Volume DeficitJeanineReyes44% (9)
- NCP-Deficient Fluid VolumeDocument1 pageNCP-Deficient Fluid Volumejanmichael8No ratings yet
- NCP For Deficient Fluid VolumeDocument2 pagesNCP For Deficient Fluid VolumeRedwing_Dc_854758% (12)
- NCP-Fluid Volume DeficitDocument2 pagesNCP-Fluid Volume Deficitjava_biscocho122979% (33)
- Nursing Care Plan for Fluid Volume DeficitDocument2 pagesNursing Care Plan for Fluid Volume DeficitXtinego89% (9)
- Nursing Care Plan Cues Diagnosis Justification: Sodium-132 Mmol/l (Low)Document3 pagesNursing Care Plan Cues Diagnosis Justification: Sodium-132 Mmol/l (Low)rei_alina75% (4)
- NCP-Fluid Volume DeficitDocument2 pagesNCP-Fluid Volume Deficitanon_207994234100% (1)
- Provide Ensuresbedside comfort,commode as privacy andneeded. convenience for patientDocument4 pagesProvide Ensuresbedside comfort,commode as privacy andneeded. convenience for patientImang Dela Cruz100% (9)
- NCP Deficient Fluid Volume Related To Fluid Loss DHNDocument2 pagesNCP Deficient Fluid Volume Related To Fluid Loss DHNMa. Elaine Carla Tating38% (8)
- NCP (Diarrhea)Document2 pagesNCP (Diarrhea)Rodj Bilang Jr.83% (30)
- Diarrhea NCPDocument3 pagesDiarrhea NCPCharles Michael Azagra0% (1)
- NCP Pediatric (Diarrhea and Impaired Mucous Membrane)Document8 pagesNCP Pediatric (Diarrhea and Impaired Mucous Membrane)Flauros Ryu Jabien60% (5)
- NCP Fluid Volume DeficitDocument2 pagesNCP Fluid Volume DeficitRez Apego0% (1)
- NCP On Electrolyte ImbalanceDocument4 pagesNCP On Electrolyte Imbalancefreyah_bc67% (3)
- Risk For Deficient Fluid Volume - NCPDocument2 pagesRisk For Deficient Fluid Volume - NCPAyla Mar100% (1)
- NCP Fluid and Electrolyte ImbalanceDocument3 pagesNCP Fluid and Electrolyte ImbalanceVitha100% (1)
- Short Term: Independent: Independent: Short TermDocument2 pagesShort Term: Independent: Independent: Short TermAndre ImperialNo ratings yet
- Assessing and Treating Acute Gastroenteritis and DehydrationDocument2 pagesAssessing and Treating Acute Gastroenteritis and DehydrationvicenteturasNo ratings yet
- Diarrhea NCPDocument2 pagesDiarrhea NCPNoriel FabrosNo ratings yet
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel100% (2)
- NCP-Risk For Fluid Volume DeficitDocument3 pagesNCP-Risk For Fluid Volume DeficitJai Go100% (1)
- NCP For DehydrationDocument3 pagesNCP For Dehydrationpeter_degamo200025% (4)
- NCP For DehydrationDocument1 pageNCP For Dehydrationjxhel63% (8)
- NCP DiarrheaDocument6 pagesNCP DiarrheaJM33% (3)
- Fluid Volume ExcessDocument2 pagesFluid Volume ExcessRodel Yacas100% (5)
- Male Patient Treatment for DehydrationDocument2 pagesMale Patient Treatment for DehydrationJamie Lee100% (2)
- Nursing Care for Gastroenteritis PatientDocument10 pagesNursing Care for Gastroenteritis PatientJoia De LeonNo ratings yet
- Nursing Care Plans for Dengue PatientDocument8 pagesNursing Care Plans for Dengue PatientCarren Wingwash100% (3)
- Fluid Volume DeficitDocument3 pagesFluid Volume Deficitprickybiik100% (1)
- NCP - Fluid and Electrolyte ImbalanceDocument3 pagesNCP - Fluid and Electrolyte ImbalancePaolo Belleza78% (9)
- Nursing Diagnosis of Fluid Volume ExcessDocument4 pagesNursing Diagnosis of Fluid Volume ExcessTamil Villardo100% (2)
- NCP DysuriaDocument1 pageNCP DysuriaJerico Geronimo DacutNo ratings yet
- Nursing Care Plan Renal FailureDocument2 pagesNursing Care Plan Renal FailureMark Jason Rabadan100% (1)
- NCP DehydrationDocument4 pagesNCP DehydrationYnah Sayoc100% (2)
- Nursing Care Plan AGNDocument2 pagesNursing Care Plan AGNAlexis Coronado50% (2)
- Fluid Volume Deficit BatuDocument2 pagesFluid Volume Deficit Batumecz26No ratings yet
- NCP. Deficient Fluid Volume by Eben D.C.Document1 pageNCP. Deficient Fluid Volume by Eben D.C.dominoredwing2024100% (1)
- Fluid Volume Excess (CRF)Document4 pagesFluid Volume Excess (CRF)NursesLabs.com100% (1)
- Risk For Deficient Fluid Volume Best NCPDocument2 pagesRisk For Deficient Fluid Volume Best NCPMikko Anthony Pingol Alarcon83% (46)
- NCP - Excess Fluid Volume (Aortic Stenosis)Document3 pagesNCP - Excess Fluid Volume (Aortic Stenosis)Daniel Vergara Arce100% (3)
- Nursing Care Plan Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective: Objective: STG: at The End of 1 DependentDocument1 pageNursing Care Plan Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective: Objective: STG: at The End of 1 DependentThomas FarrishNo ratings yet
- Subjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Document5 pagesSubjective Data: Long Term Goal: Diagnostic:: "I Was Trying To Vomit in The Emergency Department."Erle Gray CadangenNo ratings yet
- Managing Overweight through Diet and ExerciseDocument17 pagesManaging Overweight through Diet and ExerciseMarie Ashley CasiaNo ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Nursing Care PlansDocument31 pagesNursing Care PlansCyril Jane Caanyagan AcutNo ratings yet
- ROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPDocument6 pagesROSABIA, Micaela Pauline J. .-BSN-2A-ISDH-GS-NURSERY-NCPkimberly quitonNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJobelyn TunayNo ratings yet
- NCP Peptic Ulcer DsDocument4 pagesNCP Peptic Ulcer Dsplug0650% (10)
- NCP Deficit Fluid VolumeDocument4 pagesNCP Deficit Fluid VolumeKingJayson Pacman06No ratings yet
- Nursing Care Plans for Fluid Volume and Fatigue ManagementDocument4 pagesNursing Care Plans for Fluid Volume and Fatigue ManagementGILIANNE MARIE JIMENEANo ratings yet
- HydroceleDocument10 pagesHydroceleRyan ReNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- Cues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale EvaluationCharles Dave AgustinNo ratings yet
- ASSESSMENT OUTCOMES INTERVENTIONS RATIONALE EVALUATIONDocument4 pagesASSESSMENT OUTCOMES INTERVENTIONS RATIONALE EVALUATIONArian May Marcos100% (1)
- Cues Nursing Diagnosis Background and Knowledge Goals and Objectives Nursing Intervention and Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Background and Knowledge Goals and Objectives Nursing Intervention and Rationale EvaluationKristiene Kyle AquinoNo ratings yet
- Assessment Explanation of The Problem Objective Intervention Rationale Evaluation Subjective: Objective: Sto: DX StoDocument2 pagesAssessment Explanation of The Problem Objective Intervention Rationale Evaluation Subjective: Objective: Sto: DX StoBasema HashhashNo ratings yet
- NCP Deficient Fluid VolumeDocument3 pagesNCP Deficient Fluid VolumeDoneva Lyn MedinaNo ratings yet
- Renal Failure NCPDocument3 pagesRenal Failure NCPjsksNo ratings yet
- Health Teaching (Stabbed WND)Document2 pagesHealth Teaching (Stabbed WND)Jesse James Advincula EdjecNo ratings yet
- Paracetamol (Alvedon) Acetylcysteine Fluimucil KCL (Kalium Durule)Document1 pageParacetamol (Alvedon) Acetylcysteine Fluimucil KCL (Kalium Durule)Jesse James Advincula EdjecNo ratings yet
- Appendicits Case Study LATEST CHANGESDocument25 pagesAppendicits Case Study LATEST CHANGESJesse James Advincula Edjec100% (12)
- Kawasaki Disease-Case-Study LATEST CHANGESDocument24 pagesKawasaki Disease-Case-Study LATEST CHANGESJesse James Advincula Edjec100% (7)
- GEN3051 Lecture 1: Human Genes and Human Genetic DisordersDocument5 pagesGEN3051 Lecture 1: Human Genes and Human Genetic DisordersAlessander Leyendecker JuniorNo ratings yet
- QC ABO RH BloodDocument62 pagesQC ABO RH BloodrhoderickNo ratings yet
- Kabole 2023Document12 pagesKabole 2023Omoding EmmanuelNo ratings yet
- Snakes of The World A Supplement by Boundy Jeff WallachDocument284 pagesSnakes of The World A Supplement by Boundy Jeff WallachRoullienNo ratings yet
- Thermodynamics - Biotech & Bioprocess EngineeringDocument23 pagesThermodynamics - Biotech & Bioprocess EngineeringAaron Tan ShiYiNo ratings yet
- Bioteknologi: Epi Supri Wardi, M.Si Universitas Perintis Indonesia (UPERTIS) Padang, 2021Document28 pagesBioteknologi: Epi Supri Wardi, M.Si Universitas Perintis Indonesia (UPERTIS) Padang, 2021Mezi ZhahriNo ratings yet
- Cadmium Tolerance in Schinus Molle Trees Is Modulated by Enhanced Leaf Anatomy and PhotosynthesisDocument8 pagesCadmium Tolerance in Schinus Molle Trees Is Modulated by Enhanced Leaf Anatomy and PhotosynthesisPaulinho TemoteoNo ratings yet
- NM Annual Report 2011Document68 pagesNM Annual Report 2011Ni ÑoNo ratings yet
- Clinical - Biochemistry 1Document45 pagesClinical - Biochemistry 1mqbljbr529No ratings yet
- Chemistry in Everyday LifeDocument14 pagesChemistry in Everyday LifeAkhil NandanNo ratings yet
- Concept Strengthening Sheet (CSS-01) Based On AIATS-01 RMDocument19 pagesConcept Strengthening Sheet (CSS-01) Based On AIATS-01 RMB54 Saanvi SinghNo ratings yet
- 1-s2.0-S1521694210000884-Main - Epidemiology - Low Back Pain - Hoy Et Al - 2010Document13 pages1-s2.0-S1521694210000884-Main - Epidemiology - Low Back Pain - Hoy Et Al - 2010kaoxsk8No ratings yet
- Microb Monitor 2 Instructions UseDocument5 pagesMicrob Monitor 2 Instructions UseArluky NovandyNo ratings yet
- American Journal of Agricultural EconomicsDocument3 pagesAmerican Journal of Agricultural EconomicsRey DoankNo ratings yet
- 4.1.3 - State of The Australian Environment - StudentDocument5 pages4.1.3 - State of The Australian Environment - StudentMatthew Pringle100% (1)
- Developmental Psychology 1st Edition Keil Test BankDocument16 pagesDevelopmental Psychology 1st Edition Keil Test Bankstevenwhitextsngyadmk100% (29)
- Wbi15 01 Que 20231024Document36 pagesWbi15 01 Que 20231024MuqtasidNo ratings yet
- Attitude, Personality, PerceptionDocument36 pagesAttitude, Personality, PerceptionHappiness GroupNo ratings yet
- Evalution ReportDocument44 pagesEvalution ReportkamilNo ratings yet
- Love & MedicineDocument126 pagesLove & MedicinetheintrepiddodgerNo ratings yet
- Beckman ProtocolDocument34 pagesBeckman ProtocolIonut NeagaNo ratings yet
- C.6 The Nitrogen and Phosphorus Cycles (AHL) : Essential Idea: Soil Cycles Are Subject To DisruptionDocument22 pagesC.6 The Nitrogen and Phosphorus Cycles (AHL) : Essential Idea: Soil Cycles Are Subject To DisruptionAna Sofia Guzman FernandezNo ratings yet
- General Biology 1 Module 6Document19 pagesGeneral Biology 1 Module 6Vienne MonroidNo ratings yet
- Banana Peel Extract Mediate Synthesis of Gold NanoparticlesDocument6 pagesBanana Peel Extract Mediate Synthesis of Gold NanoparticlesZohaib Khurshid SultanNo ratings yet
- DR Fadel Naim Ass. Prof. Faculty of Medicine IUGDocument65 pagesDR Fadel Naim Ass. Prof. Faculty of Medicine IUGأمال داودNo ratings yet
- SGS Daily Light Integral Research StudyDocument10 pagesSGS Daily Light Integral Research Studyhari HaranNo ratings yet
- Therapy PolarityDocument37 pagesTherapy PolarityNaina RavahitrarivoNo ratings yet
- PMS-poster 2 PDFDocument2 pagesPMS-poster 2 PDFKuNtii Devi VerdejofNo ratings yet
- The Neuropsychology of EmotionDocument532 pagesThe Neuropsychology of EmotionLarisa Ev-a Elena95% (43)
- Chapter 3 - Antibody Topic NotesDocument10 pagesChapter 3 - Antibody Topic NotesAngelica Joy GonzalesNo ratings yet