You might also like
- 12 OET Sample Referral Letter (Nurse) WritingDocument43 pages12 OET Sample Referral Letter (Nurse) WritingAL ' ARIS98% (41)
- q2 Grade 9 Pe DLL Week 1Document11 pagesq2 Grade 9 Pe DLL Week 1Airaa A. Baylan88% (8)
- Target Electric Blanket InstructionsDocument15 pagesTarget Electric Blanket Instructionsbritt16110% (1)
- Investigation Into The Rate of Respiration Using A SpirometerDocument10 pagesInvestigation Into The Rate of Respiration Using A SpirometerNayantara GopiNo ratings yet
- B Alert x10 User ManualDocument25 pagesB Alert x10 User ManualfrancistsyNo ratings yet
- Perfusion SystemDocument30 pagesPerfusion SystemShailendra Singh Khichi100% (1)
- Siamese-rPPG Network: Remote Photoplethysmography Signal Estimation From Face VideosDocument19 pagesSiamese-rPPG Network: Remote Photoplethysmography Signal Estimation From Face Videos李翊安No ratings yet
- Case ManagementDocument4 pagesCase ManagementPraveena.R100% (1)
- Diagnostic SpirometerDocument3 pagesDiagnostic SpirometerseventhsensegroupNo ratings yet
- MEDICAL ELECTRONICS PROJECTS ABSTRACT-Digital Pulmonary Function Test - SpirometryDocument4 pagesMEDICAL ELECTRONICS PROJECTS ABSTRACT-Digital Pulmonary Function Test - SpirometryR.ASHOKKUMAARNo ratings yet
- Diclofenac From Administration To Adverse Effect A Mini-ReviewDocument5 pagesDiclofenac From Administration To Adverse Effect A Mini-ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Coursework 1-Personal Development Plan: Student ID: Word CountDocument12 pagesCoursework 1-Personal Development Plan: Student ID: Word CountrajeshNo ratings yet
- Defibrillatorppt 131028115457 Phpapp01Document41 pagesDefibrillatorppt 131028115457 Phpapp01Simon JosanNo ratings yet
- BMI403.3 Biomedical InstrumentationDocument2 pagesBMI403.3 Biomedical InstrumentationDarpan Specchio PudasainiNo ratings yet
- Oxygen CascadeDocument12 pagesOxygen Cascadehy3pjb1984No ratings yet
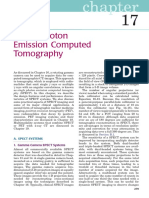
- Chapter 17 Single Photon Emission Computed TomographyDocument28 pagesChapter 17 Single Photon Emission Computed TomographyJohnnie LópezNo ratings yet
- Contrast MediaDocument6 pagesContrast MediardmdelarosaNo ratings yet
- HP Diagnosis ChallengesDocument51 pagesHP Diagnosis ChallengesskchhabraNo ratings yet
- Basic Considerations in Nuclear MedicineDocument12 pagesBasic Considerations in Nuclear Medicinechberg13No ratings yet
- 1.0 The Origin of Biopotentials (New)Document62 pages1.0 The Origin of Biopotentials (New)Hanif HussinNo ratings yet
- SAR PPT 1-Program - 07Document36 pagesSAR PPT 1-Program - 07ni60No ratings yet
- Cherenkov RadiationDocument17 pagesCherenkov RadiationMayank GargNo ratings yet
- Baska MaskDocument8 pagesBaska MaskAnish H DaveNo ratings yet
- Anesthesia Considerations for Microlaryngoscopy and Direct LaryngoscopyDocument6 pagesAnesthesia Considerations for Microlaryngoscopy and Direct LaryngoscopyRubén Darío HerediaNo ratings yet
- A History of InnovationFromNovametrix To PhilipsDocument64 pagesA History of InnovationFromNovametrix To PhilipsEdgar GodinhoNo ratings yet
- EasyOn PC ManualDocument120 pagesEasyOn PC Manualasdfasdf87No ratings yet
- Non-Invasive Glucose SensorsDocument12 pagesNon-Invasive Glucose SensorsGerman GodiNo ratings yet
- The Artificial Heart: A Design Example: BIOE 1000 October 18, 2001Document17 pagesThe Artificial Heart: A Design Example: BIOE 1000 October 18, 2001Paspulati Leelaram100% (1)
- Senior Radiographer Nuclear MedicineDocument1 pageSenior Radiographer Nuclear Medicinetafi66No ratings yet
- 65 PDFDocument7 pages65 PDFShajan SNo ratings yet
- Sample Size CalculationsDocument5 pagesSample Size CalculationsAKNTAI002100% (1)
- Vant Hof SpringerProtocols 2019 V2finalDocument38 pagesVant Hof SpringerProtocols 2019 V2finalSusi SusantiNo ratings yet
- Role of Simulation in Anesthesia PracticeDocument39 pagesRole of Simulation in Anesthesia PracticeNitin ..100% (1)
- EEGDocument16 pagesEEGadibaronessNo ratings yet
- Nuclear Medicine GuideDocument3 pagesNuclear Medicine GuidejeffsunilNo ratings yet
- BioMedical TelemetryDocument7 pagesBioMedical TelemetrySean Matthew L. OcampoNo ratings yet
- Grip Strength and ElectromyogramDocument8 pagesGrip Strength and ElectromyogramChandra Murali100% (1)
- Abebaw Research ProposalDocument32 pagesAbebaw Research ProposalDerese BishawNo ratings yet
- Nuclear Medicine Inc.'s Iodine Value Chain AnalysisDocument6 pagesNuclear Medicine Inc.'s Iodine Value Chain AnalysisPrashant NagpureNo ratings yet
- Chapter 3 - Introduction To Nuclear MedicineDocument4 pagesChapter 3 - Introduction To Nuclear MedicineunknownxemNo ratings yet
- Aeroneb Solo DFU - EN - Rev JDocument56 pagesAeroneb Solo DFU - EN - Rev Jyagnaashi9092No ratings yet
- 17 Aususgt Final ProtocolDocument22 pages17 Aususgt Final ProtocolRishabh VermaNo ratings yet
- 3-EEG Fni$Document50 pages3-EEG Fni$chanlalNo ratings yet
- Pulseless Pumps & Artificial HeartsDocument23 pagesPulseless Pumps & Artificial HeartscafemedNo ratings yet
- Guidelines For Sedation and Anesthesia in GI Endos PDFDocument11 pagesGuidelines For Sedation and Anesthesia in GI Endos PDFHernan RuedaNo ratings yet
- Ch2 BiosignalsDocument15 pagesCh2 BiosignalsDip PaulNo ratings yet
- Tissue Optics Light Scattering Methods and InstrumDocument7 pagesTissue Optics Light Scattering Methods and InstrumDaniela UrreaNo ratings yet
- Design and Prototyping of A Low-Cost Portable Mechanical - DMD - 2010 - Al - Husseini - MITDocument13 pagesDesign and Prototyping of A Low-Cost Portable Mechanical - DMD - 2010 - Al - Husseini - MITSebastian100% (1)
- Spirometry E-Guide 2013Document28 pagesSpirometry E-Guide 2013Vidal Odon Ramos MermaNo ratings yet
- Dopaminergic and Serotonergic Neurohumoural TransmissionDocument23 pagesDopaminergic and Serotonergic Neurohumoural TransmissionChaitanya Kiran PullelaNo ratings yet
- Nuclear Medicine Tehnologist or Lead Nuclear Medicine TechnologiDocument2 pagesNuclear Medicine Tehnologist or Lead Nuclear Medicine Technologiapi-78955179No ratings yet
- Receptor PhysiologyDocument34 pagesReceptor PhysiologyKarl Torres Uganiza RmtNo ratings yet
- Palm Vein Authentication - Novák PDFDocument25 pagesPalm Vein Authentication - Novák PDFSatheesh Kumar100% (1)
- SaranDocument23 pagesSaranAbhishek BNo ratings yet
- Wearable BiosensorDocument26 pagesWearable BiosensorViolet blossomNo ratings yet
- MedicalelectricalsafetyDocument89 pagesMedicalelectricalsafetyMeruva LokeshwarNo ratings yet
- 2007 PFTs The Forced Oscillation TechniqueDocument50 pages2007 PFTs The Forced Oscillation TechniqueServiço de Imunoalergologia - H.S. João100% (1)
- 1.5.0.potentials and EquilibriumDocument8 pages1.5.0.potentials and EquilibriumAnonymous G3DRjDMkNo ratings yet
- Manipulation of The Cervical Spine A Systematic Review of Case Reports of Serious Adverse Events1995-2001Document5 pagesManipulation of The Cervical Spine A Systematic Review of Case Reports of Serious Adverse Events1995-2001Carlos Martín De RosasNo ratings yet
- Insulin Pump System DesignDocument10 pagesInsulin Pump System DesignmikeNo ratings yet
- The Radiation Chemistry of MacromoleculesFrom EverandThe Radiation Chemistry of MacromoleculesMalcolm DoleNo ratings yet
- Smart Home Technologies and Services for Geriatric RehabilitationFrom EverandSmart Home Technologies and Services for Geriatric RehabilitationMohamed-Amine ChoukouNo ratings yet
- Journal ClubDocument12 pagesJournal ClubAnonymous ibmeej9No ratings yet
- Revised Jones Criteria JurdingDocument41 pagesRevised Jones Criteria JurdingddantoniusgmailNo ratings yet
- Healing Through MusicDocument11 pagesHealing Through MusicMiguel MacaroNo ratings yet
- Pramipexole Effect on Depressive Symptoms in Parkinson's DiseaseDocument6 pagesPramipexole Effect on Depressive Symptoms in Parkinson's DiseaseCarmen CiursaşNo ratings yet
- Tatalaksana Emboli Paru PerkiDocument6 pagesTatalaksana Emboli Paru PerkiEviNo ratings yet
- Price List PT - Thirza 2019Document8 pagesPrice List PT - Thirza 2019Permana JuliansyahNo ratings yet
- PYQDocument2 pagesPYQAisyah OthmanNo ratings yet
- English for Nurses: A Concise GuideDocument137 pagesEnglish for Nurses: A Concise GuideLIDYANo ratings yet
- Virtual ColonosDocument200 pagesVirtual ColonosDiana VershyninaNo ratings yet
- NLEDocument18 pagesNLEKeij AranetaNo ratings yet
- Tugas B.inggris 28 Agt 2K20 Eli Irna eDocument3 pagesTugas B.inggris 28 Agt 2K20 Eli Irna eAhmad AsrullahNo ratings yet
- AIJ Clasif PRINTO 2019Document9 pagesAIJ Clasif PRINTO 2019Michael ParksNo ratings yet
- Vyanga Synopsis1Document2 pagesVyanga Synopsis1aniketNo ratings yet
- Abses Perianal JurnalDocument4 pagesAbses Perianal JurnalAnonymous tDKku2No ratings yet
- Wardlaws Perspectives in Nutrition 9th Edition Byrd Bredbenner Test BankDocument32 pagesWardlaws Perspectives in Nutrition 9th Edition Byrd Bredbenner Test Bankedricduyenuc1uw100% (19)
- Nama: Riris Putri Marito Sinaga NIM: 04022722125001 Prodi: Ilmu Kesehatan Anak No Soal 35Document13 pagesNama: Riris Putri Marito Sinaga NIM: 04022722125001 Prodi: Ilmu Kesehatan Anak No Soal 35Riris SinagaNo ratings yet
- Heart Disease in Pregnancy GuideDocument3 pagesHeart Disease in Pregnancy GuideNasehah SakeenahNo ratings yet
- NCMB317 Lec MidtermDocument55 pagesNCMB317 Lec Midterm2 - GUEVARRA, KYLE JOSHUA M.No ratings yet
- The Complete Enema Guide: by Helena BinghamDocument10 pagesThe Complete Enema Guide: by Helena BinghamJ.J.No ratings yet
- Embarazo y Ae PDFDocument13 pagesEmbarazo y Ae PDFraquel lopezNo ratings yet
- Pfin 6th Edition Billingsley Test BankDocument24 pagesPfin 6th Edition Billingsley Test BankNatalieRojasykebg100% (32)
- First Aid and Water SurvivalDocument18 pagesFirst Aid and Water SurvivalKri de Asis83% (12)
- Transcript 247 Pectasol C Modified Citrus Pectin and The Toxins It Removes With Dr. Isaac EliazDocument16 pagesTranscript 247 Pectasol C Modified Citrus Pectin and The Toxins It Removes With Dr. Isaac EliazField90No ratings yet
- Cardiovascular Physiology Applied To Critical Care and AnesthesiDocument12 pagesCardiovascular Physiology Applied To Critical Care and AnesthesiLuis CortezNo ratings yet
- APA Eating Disorders Practice Guideline Under CopyeditingDocument139 pagesAPA Eating Disorders Practice Guideline Under CopyeditingIbrahim NasserNo ratings yet
- Atom Electrosurgical SystemDocument40 pagesAtom Electrosurgical SystemOgut AjaNo ratings yet
- Physical Exam of the Eye: Structures, Findings, DiagnosesDocument16 pagesPhysical Exam of the Eye: Structures, Findings, DiagnosesriveliNo ratings yet