You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tromboza VenoasaDocument4 pagesTromboza VenoasaDanielaNo ratings yet
- 09 Acute Med AbdDocument42 pages09 Acute Med AbdDanielaNo ratings yet
- Dislipidemii Vlad 2011Document40 pagesDislipidemii Vlad 2011DanielaNo ratings yet
- Pulmonary ThromboembolismDocument25 pagesPulmonary ThromboembolismDanielaNo ratings yet
- 07 The Valvular PatientDocument83 pages07 The Valvular PatientDanielaNo ratings yet
- 12 Hemorrhagic SyndromesDocument16 pages12 Hemorrhagic SyndromesDanielaNo ratings yet
- Early Diagnosis of NeoplasisDocument25 pagesEarly Diagnosis of NeoplasisDanielaNo ratings yet
- 2007 Engleza Heart FailureDocument38 pages2007 Engleza Heart FailureDanielaNo ratings yet
- Urologic and Nephrologic DisordersDocument49 pagesUrologic and Nephrologic DisordersDanielaNo ratings yet
- 11 Gastrointestinal DiseasesDocument32 pages11 Gastrointestinal DiseasesDanielaNo ratings yet
- 12 AnaemiasDocument52 pages12 AnaemiasDanielaNo ratings yet
- BraziliaDocument1 pageBraziliamamaluiraresNo ratings yet
- 05 Patient With Acute Thoracic PainDocument69 pages05 Patient With Acute Thoracic PainDanielaNo ratings yet
- 04 Patient With HypertensionDocument47 pages04 Patient With HypertensionDanielaNo ratings yet
- The Patient With Fever: Assoc. Prof. Simona DraganDocument29 pagesThe Patient With Fever: Assoc. Prof. Simona DraganDanielaNo ratings yet
- It Ali ADocument1 pageIt Ali ADanielaNo ratings yet
- Argent in ADocument1 pageArgent in ADanielaNo ratings yet
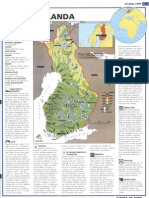
- Finland ADocument1 pageFinland AmamaluiraresNo ratings yet
- HTAcursDocument44 pagesHTAcursDanielaNo ratings yet
- Delegation TreeDocument2 pagesDelegation TreeKatie_Poindext_5154100% (1)
- Malignant Struma OvariiDocument4 pagesMalignant Struma Ovariixwahyu 108No ratings yet
- CBinsights Global Healthcare Report Q2 2019Document70 pagesCBinsights Global Healthcare Report Q2 2019Andre Matsushima TeixeiraNo ratings yet
- Jayden Alexander Tirta - Speech PreparationDocument5 pagesJayden Alexander Tirta - Speech PreparationJAYDEN ALEXANDER TIRTANo ratings yet
- GANG FIT (Part 2)Document58 pagesGANG FIT (Part 2)John WangNo ratings yet
- Oral Sex - A Closer LookDocument9 pagesOral Sex - A Closer LookiantorresNo ratings yet
- U03d2 Ethics, Recruitment, and Random AssignmentDocument6 pagesU03d2 Ethics, Recruitment, and Random Assignmentarhodes777No ratings yet
- Geriatrics Prescribing GuidelinessDocument27 pagesGeriatrics Prescribing GuidelinessSayli Gore100% (1)
- Final Report KEF NGO Vismay NaikDocument14 pagesFinal Report KEF NGO Vismay NaikVismay NaikNo ratings yet
- VaanannanDocument53 pagesVaanannankevalNo ratings yet
- Preoperative Evaluation ChecklistDocument7 pagesPreoperative Evaluation ChecklistPiny Elleine CesarNo ratings yet
- PANDEMICS Mary Shelley, The Cumaen Sibyl and The Last ManDocument19 pagesPANDEMICS Mary Shelley, The Cumaen Sibyl and The Last ManSue Bradley100% (2)
- Medicina Natural GatosDocument40 pagesMedicina Natural GatosfdfdfdfNo ratings yet
- Lower Gastrointestinal Bleeding: Practice EssentialsDocument28 pagesLower Gastrointestinal Bleeding: Practice EssentialsJohnPaulOliverosNo ratings yet
- Metabolic AftershockDocument36 pagesMetabolic AftershockVicWoods0% (1)
- The Diabetic FootDocument33 pagesThe Diabetic Footpagar bersihNo ratings yet
- Health & SafetyDocument6 pagesHealth & Safetykamran alamNo ratings yet
- To Define Clinical Psychology, Here Is A Definition From American Psychological Association's Division 12Document14 pagesTo Define Clinical Psychology, Here Is A Definition From American Psychological Association's Division 12Summer LoveNo ratings yet
- MIT Medical Department Pediatrics History Form: AppointmentDocument4 pagesMIT Medical Department Pediatrics History Form: Appointmentmaddythedoc100% (1)
- The ICF-CY model as a framework for pediatric rehabilitationDocument2 pagesThe ICF-CY model as a framework for pediatric rehabilitationAtet KurniadiNo ratings yet
- Lesson PlanDocument3 pagesLesson PlanRenato Torio100% (1)
- Bac Level: Beer Is A Beverage FermentedDocument2 pagesBac Level: Beer Is A Beverage FermentedBea ToleteNo ratings yet
- Hormone Therapy IfmDocument16 pagesHormone Therapy IfmRamy LasheenNo ratings yet
- MFHSISDocument1 pageMFHSIShanchee leeNo ratings yet
- M.T. Villanueva Avenue, Naga City: Naga College Foundation First Semester S/Y 2019-2020Document6 pagesM.T. Villanueva Avenue, Naga City: Naga College Foundation First Semester S/Y 2019-2020junalynNo ratings yet
- Compensation Fy2018sDocument218 pagesCompensation Fy2018sJesse YoungbloodNo ratings yet
- Abilify Drug Study: Therapeutic Effects, Indications, Contraindications and Adverse ReactionsDocument6 pagesAbilify Drug Study: Therapeutic Effects, Indications, Contraindications and Adverse ReactionsLuige AvilaNo ratings yet
- Marjory GordonDocument7 pagesMarjory GordonPusimah IsmayfiNo ratings yet
- 17 SDGsDocument48 pages17 SDGsKiều Ngọc DungNo ratings yet
- Elimination Diet Guide Reveals Surprising Health Problems Caused by Food SensitivitiesDocument1 pageElimination Diet Guide Reveals Surprising Health Problems Caused by Food Sensitivitiesgianluca136No ratings yet