You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Blood Supply of Long BonesDocument4 pagesBlood Supply of Long BonesmainehoonaNo ratings yet
- Osteomyelitis: Dr. Sunil Pahari 2 Year Resident Department of Orthopedics Yangtze UniversityDocument48 pagesOsteomyelitis: Dr. Sunil Pahari 2 Year Resident Department of Orthopedics Yangtze UniversityPercy Linares MorilloNo ratings yet
- RT 112 Module 2Document67 pagesRT 112 Module 2AVE MAE ALEXIS NAVATANo ratings yet
- Cancer and Oncology Nursing NCLEX Practice Quiz ANSDocument5 pagesCancer and Oncology Nursing NCLEX Practice Quiz ANSyanyan cadizNo ratings yet
- 6 Kuliah Radiology of MSKDocument46 pages6 Kuliah Radiology of MSKDesak PratiwiNo ratings yet
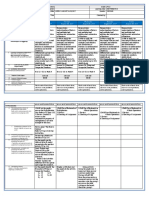
- Q2 W1 DLL For August 14-18-2017 All SubjectsDocument42 pagesQ2 W1 DLL For August 14-18-2017 All SubjectsJess MaglunobNo ratings yet
- Fracture Management in Avian Species: Daniel Calvo CarrascoDocument16 pagesFracture Management in Avian Species: Daniel Calvo CarrascoJessica RuizNo ratings yet
- Testing "Saintly" Authenticity: Investigations On Two Catacomb SaintsDocument8 pagesTesting "Saintly" Authenticity: Investigations On Two Catacomb SaintsRed OdisseyNo ratings yet
- Healing of FracturesDocument19 pagesHealing of FracturesTracy100% (4)
- What Is The Ewing Family of Tumors?Document43 pagesWhat Is The Ewing Family of Tumors?rantiayefNo ratings yet
- Pediatric Bone Imaging Differentiating Benign Lesions From MalignantDocument9 pagesPediatric Bone Imaging Differentiating Benign Lesions From MalignantElshaer MohammedNo ratings yet
- Oral Histology NotesDocument18 pagesOral Histology NotesKhalil Raziq100% (1)
- Intramembranous Ossification & Endochondral Ossification PDFDocument41 pagesIntramembranous Ossification & Endochondral Ossification PDFKayla Joezette100% (1)
- Drugs in Orthodontics: G.Shekar Subramanian Ist Year PGDocument69 pagesDrugs in Orthodontics: G.Shekar Subramanian Ist Year PGShekar SubramanianNo ratings yet
- 2018 CSB520 ANSWERS Skeletal System PathologyDocument4 pages2018 CSB520 ANSWERS Skeletal System PathologyNathanNo ratings yet
- Metabolic Bone ConditionsDocument66 pagesMetabolic Bone ConditionsNaeem AminNo ratings yet
- Tsubota 2009Document7 pagesTsubota 2009Catherine NocuaNo ratings yet
- Dr. Namrata .A (B.A.M.S - Mumbai)Document23 pagesDr. Namrata .A (B.A.M.S - Mumbai)kalloornatorNo ratings yet
- Reading PassagesDocument8 pagesReading PassagesHoàng NguyễnNo ratings yet
- Zuogui Wan (左归丸) improves trabecular bone microarchitecture in ovariectomy-induced osteoporosis rats by regulating orexin-A and orexin receptorsDocument8 pagesZuogui Wan (左归丸) improves trabecular bone microarchitecture in ovariectomy-induced osteoporosis rats by regulating orexin-A and orexin receptorsHùng Nguyễn ĐìnhNo ratings yet
- Bone and Soft Tissue PathologyDocument47 pagesBone and Soft Tissue PathologyDebo AdeosoNo ratings yet
- Hip DislocationDocument39 pagesHip DislocationJordan Garcia Aguilar0% (1)
- 206 Bones in Human BodyDocument7 pages206 Bones in Human BodyChelsea MarieNo ratings yet
- Age-Dependent Biologic Response To Orthodontic Forces: Original ArticleDocument13 pagesAge-Dependent Biologic Response To Orthodontic Forces: Original ArticleAnushriya DuttaNo ratings yet
- Bio-Hybrid Implant, Next Generation of Bio-Engineered Implant - A ReviewDocument9 pagesBio-Hybrid Implant, Next Generation of Bio-Engineered Implant - A ReviewPartha Sarathi AdhyaNo ratings yet
- The Importance of Friendship EssayDocument6 pagesThe Importance of Friendship Essayafibojmbjifexj100% (2)
- Orthopedics BoneDisordersDocument20 pagesOrthopedics BoneDisordersannapanna1No ratings yet
- Cell SaltsDocument8 pagesCell SaltsminunatNo ratings yet
- Johnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-261-280Document20 pagesJohnson Jerry Alan Chinese Medical Qigong Therapy Vol 5-261-280toanbauNo ratings yet
- Bio IntegrationDocument126 pagesBio IntegrationIan CostaNo ratings yet