BMC Infectious Diseases
Research article
BioMed Central
Open Access
Male circumcision, religion, and infectious diseases: an ecologic analysis of 118 developing countries
Paul K Drain1, Daniel T Halperin*2, James P Hughes3, Jeffrey D Klausner4 and Robert C Bailey5
Address: 1University of Washington School of Medicine, Seattle, USA, 2United States Agency for International Development, Southern Africa Regional HIV-AIDS Program, Mbabane, Swaziland, 3Center for AIDS and STD, University of Washington, Seattle, USA, 4San Francisco Department of Public Health, San Francisco, USA and 5Division of Epidemiology, University of Illinois at Chicago, Chicago, USA Email: Paul K Drain - pkdrain@u.washington.edu; Daniel T Halperin* - dhalperin@usaid.gov; James P Hughes - jphughes@u.washington.edu; Jeffrey D Klausner - jeff.klausner@sfdph.org; Robert C Bailey - rcbailey@uic.edu * Corresponding author
Published: 30 November 2006 BMC Infectious Diseases 2006, 6:172 doi:10.1186/1471-2334-6-172
Received: 07 April 2006 Accepted: 30 November 2006
This article is available from: http://www.biomedcentral.com/1471-2334/6/172 2006 Drain et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Both religious practices and male circumcision (MC) have been associated with HIV and other sexually-transmitted infectious diseases. Most studies have been limited in size and have not adequately controlled for religion, so these relationships remain unclear. Methods: We evaluated relationships between MC prevalence, Muslim and Christian religion, and 7 infectious diseases using country-specific data among 118 developing countries. We used multivariate linear regression to describe associations between MC and cervical cancer incidence, and between MC and HIV prevalence among countries with primarily sexual HIV transmission. Results: Fifty-three, 14, and 51 developing countries had a high (>80%), intermediate (2080%), and low (<20%) MC prevalence, respectively. In univariate analyses, MC was associated with lower HIV prevalence and lower cervical cancer incidence, but not with HSV-2, syphilis, nor, as expected, with Hepatitis C, tuberculosis, or malaria. In multivariate analysis after stratifying the countries by religious groups, each categorical increase of MC prevalence was associated with a 3.65/100,000 women (95% CI 0.54-6.76, p = 0.02) decrease in annual cervical cancer incidence, and a 1.84-fold (95% CI 1.36-2.48, p < 0.001) decrease in the adult HIV prevalence among sub-Saharan African countries. In separate multivariate analyses among non-sub-Saharan African countries controlling for religion, higher MC prevalence was associated with a 8.94-fold (95% CI 4.30-18.60) decrease in the adult HIV prevalence among countries with primarily heterosexual HIV transmission, but not, as expected, among countries with primarily homosexual or injection drug use HIV transmission (p = 0.35). Conclusion: Male circumcision was significantly associated with lower cervical cancer incidence and lower HIV prevalence in sub-Saharan Africa, independent of Muslim and Christian religion. As predicted, male circumcision was also strongly associated with lower HIV prevalence among countries with primarily heterosexual HIV transmission, but not among countries with primarily homosexual or injection drug use HIV transmission. These findings strengthen the reported biological link between MC and some sexually transmitted infectious diseases, including HIV and cervical cancer.
Page 1 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
Background
Geographical variations in HIV prevalence have been observed between less-developed and more-developed countries, as well as within regions of similar socioeconomic development [1-5]. The epidemiology of HIV and other infectious diseases have been associated with both religious practices and male circumcision [1-19]. Religious beliefs and practices dictate many societal and sexual behaviors that influence transmission of sexuallytransmitted infections (STIs) [20]. Male circumcision has been more common among populations with lower rates of HIV, cervical cancer, and other STIs [3,10-13], and shown in one randomized trial to reduce HIV transmission [21]. Although religious affiliation is a major determinant of male circumcision status [12], many analyses have not controlled for religion when examining relationships between male circumcision and infectious diseases. This study builds upon and further expands our previously reported analyses of variables associated with country-specific HIV prevalence and cervical cancer incidence [5,22]. In our extensive analysis of HIV co-factors, among 81 variables male circumcision had the strongest association with HIV prevalence [5]. We now present a more thorough examination of the association between male circumcision and HIV prevalence by better adjusting for religion, by separately analyzing the sub-Saharan African region, and by conducting separate analyses between countries with sexual versus non-sexual primary modes of HIV transmission. Our previous ecological analysis of cervical cancer utilized 54 country-level variables, but did not include the important determinant of male circumcision [13,22]. We complete our previous analysis by describing the relationships between male circumcision and cervical cancer, and by including male circumcision in the previously reported multivariate model. In addition, we further expand on our previous studies by describing the epidemiology of male circumcision among developing countries and by describing associations between male circumcision and five other infectious diseases.
subsequent country-specific data were collected for 122 low and medium human development ("developing") countries.
Data collection The Joint United Nations Programme on HIV/AIDS (UNAIDS) provided country-specific age-standardized HIV seroprevalence per 100 adults 1549 years old for the year 2004 for 100 countries [24]. Countries with <0.1% of adults infected with HIV were considered to have an adult seroprevalence of 0.05%. The International Agency for Research on Cancer provided country-specific annual agestandardized cervical cancer incidence [a surrogate measure for Human Papillomavirus (HPV)] per 100,000 females for the year 2000 for 117 countries and the most recent country-specific Herpes Simplex Virus type-2 (HSV2) seroprevalence per 100 women for 23 countries [25,26]. The World Health Organization provided the most recent country-specific syphilis seroprevalence per 10,000 women for 43 countries [27], and Hepatitis C prevalence per 100 adults for 75 countries [28]. The UNDP provided country-specific prevalence of all forms of tuberculosis per 100,000 people for the year 2002 for 110 countries and malaria prevalence per 10,000 people for the year 2000 for 94 countries [23]. We did not include chlamydia or gonorrhea in this analysis due to a lack of available data.
Methods
We conducted an ecological study of country-level variables among developing countries. The United Nations Development Programme (UNDP) 'Human Development Report 2004' provided the Human Development Index, which determines each country's development status on the basis of life expectancy, educational attainment, and adjusted real income [23]. Countries classified as high human development ("developed") countries were excluded from the analyses under the assumption that they have greater capacity to sustain national treatment and prevention programs, and have different epidemiological infectious disease profiles. Therefore,
We used survey data from various published sources [3,11-13,15,29,30], including Demographic and Health Surveys and Behavioral Surveillance Surveys [31-35] to categorize the country-wide prevalence of male circumcision as "low" (<20%), "intermediate" (2080%), or "high" (>80%), as we have previously done [5,10]. These categories were chosen to best minimize misclassification. When published country-specific data were not available, we used ethnographic confidence methods, as previously utilized by Halperin and Bailey [5,10], to categorize country-specific male circumcision prevalence as low, intermediate, or high. The classification of country-specific male circumcision prevalence was independently verified by three colleagues (listed in Acknowledgements). We omitted four developing countries (Armenia, Belarus, Kyrgyzstan, and Vanuatu) from all analyses because their male circumcision prevalence could not be confidently categorized. The United Nations Population Division provided all population statistics estimated for the year 2000 [36]. UNAIDS provided data for geographical regions [24]. We used the first listed mode of transmission from the UNAIDS 'HIV/AIDS Epidemic Update 2002' as the primary mode of HIV transmission for each geographical region [37]. The United States Central Intelligence Agency 'The World Factbook' provided both the percentage of
Page 2 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
Muslims and the percentage of Christians within each country [38].
Statistical analyses Statistical analyses were conducted on 118 developing countries using Stata Version 8.0 [39]. All regression statistics were performed using a robust variance to account for unmeasured ecologic and population differences. We conducted separate analyses of HIV prevalence among sub-Saharan African and non-sub-Saharan African countries due to the differing severity and nature of the epidemics [40-42]. We also conducted separate analyses among non-sub-Saharan African regions whose primary mode of HIV transmission was heterosexual contact versus homosexual contact or injection drug use [24]. Heterosexual contact was the primary mode of HIV transmission for the sub-Saharan African region. HIV seroprevalence was natural log (ln)-transformed to create a more normal distribution for regression analyses. Countries were categorized into tertiles as having low (<5%), intermediate (555%), and high (>55%) percentage of predominantly Muslims, and as having low (<6%), intermediate (655%), and high (>55%) percentage of predominantly Christians.
cancer incidence. Definitions and sources of these variables (number of doctors per 100,000 people, percent of children immunized for measles, female disabilityadjusted life expectancy in years, percent of female adult illiteracy rate, percent of infants with low birth weight, and geographic region as defined by the International Agency for Research on Cancer), have been previously described [22]. Similarly, a multivariate model of HIV prevalence was conducted adjusting for the 6 additional variables that were previously found to be significant (p < 0.05) indicators of HIV prevalence. Detailed methods, including definitions and sources of these variables (years since HIV was first reported, geographic region, percent of the population younger than 25 years, percent of female adult illiteracy rate, percent of children fully immunized for diphtheria, tetanus, and pertussis, and number of doctors per 100,000 people), have been previously described [5].
Results
Male circumcision prevalence The classification of male circumcision prevalence is listed in Table 1 for 118 developing countries. Among these, 53 countries, containing 700 million males, were categorized as having a high (>80%) male circumcision prevalence, 14 countries, containing 135 million males, were categorized as having an intermediate (2080%) male circumcision prevalence, and 51 countries, containing 1.6 billion males, were categorized as having a low (<20%) male circumcision prevalence.
The mean and standard deviation for each infectious disease were separately summarized among countries with low and high male circumcision prevalence. Means and standard deviations for cervical cancer incidence and HIV prevalence were also separately summarized among countries with low and high male circumcision prevalence within each religious tertile group. Means and standard deviations were analyzed for statistical significance between high versus low male circumcision groups using 2-sample t tests for independent samples with unequal variances. Univariate linear regression statistics examined category of male circumcision prevalence with each infectious disease. Results are presented by order of the R2 value, which estimates the amount of the variance explained by the association. Since only HIV prevalence and cervical cancer incidence were significantly associated with male circumcision in univariate analyses, subsequent multivariate analyses were only performed for these two outcomes. Multivariate analyses of covariance models included each country's percentage of the population Muslim and percentage of the population Christian. Additional multivariate analyses were conducted for cervical cancer incidence and HIV prevalence based on our previously published models [5,22]. In brief, a multivariate model of cervical cancer incidence was conducted adjusting for the 6 additional variables that were previously found to be significant (p < 0.05) indicators of cervical
Male circumcision prevalence had a distinct geographical pattern. Thirteen of 14 (93%) developing countries in North Africa and the Middle East had a high male circumcision prevalence. Twenty-eight of 45 (62%) sub-Saharan African countries had a high male circumcision prevalence. Eight of 27 (30%) Southeast Asian and Pacific Island countries had a high male circumcision prevalence, and most circumcised males resided in Indonesia, Pakistan, Bangladesh, or the Philippines. Only 4 of 18 (22%) developing countries in Europe and Central Asia had a high male circumcision prevalence, and all 18 developing countries in Latin American and the Caribbean region had a low male circumcision prevalence.
Male circumcision and religion As expected, male circumcision was strongly associated with religious variables (data not presented). A greater percent of the population being Muslim was strongly associated with more male circumcision prevalence (p < 0.001). Conversely, a greater percent of the population being Christian was strongly associated with less male circumcision (p < 0.001). Among 49 countries with high male circumcision prevalence, the mean percentage of the
Page 3 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
Table 1: Category of male circumcision prevalence for 118 developing countries.
Male Circumcision Prevalence Low (<20%) Belize Bhutan Bolivia Botswana Brazil Bulgaria Burundi Cambodia Cape Verde China Colombia Dominican Republic Ecuador El Salvador Fiji French Polynesia Georgia Guatemala Guyana Haiti Honduras India Jamaica Korea, DPR Lao, PDR Malawi Micronesia, Fed States Moldova, Rep of Mongolia Myanmar Namibia Nepal Nicaragua Panama Papua New Guinea Paraguay Peru Romania Russian Federation Rwanda Samoa Solomon Islands Sri Lanka Suriname Swaziland Thailand Ukraine Venezuela Viet Nam Zambia Zimbabwe Intermediate (2080%) Albania Bosnia Herzegovina Central African Republic Cote d'Ivoire Ethiopia Kazakhstan Lesotho Macedonia, FYR of Mozambique South Africa Sudan Tanzania, United Rep of Uganda Yugoslavia High (>80%) Afghanistan Algeria Angola Azerbaijan Bangladesh Benin Burkina Faso Cameroon Chad Comoros Congo (Brazzaville) Dem Rep of the Congo Djibouti Egypt Equatorial Guinea Eritrea Gabon Gambia Ghana Guinea Guinea-Bissau Indonesia Iran, Islam Rep of Iraq Jordan Kenya Lebanon Liberia Libyan Arab Jama Madagascar Malaysia Maldives Mali Mauritania Mauritius Morocco Niger Nigeria Oman Pakistan Philippines Saudi Arabia Senegal Sierra Leone Somalia Syrian Arab Rep Tajikistan Togo Tunisia Turkey Turkmenistan Uzbekistan Yemen
population Muslim was 69% and the mean percentage of the population Christian was 16%.
Male circumcision and infectious diseases In univariate regression analyses, male circumcision was associated with HIV prevalence among sub-Saharan African countries, HIV prevalence among non-sub-Saharan African countries with primarily heterosexual contact, HIV prevalence among non-sub-Saharan countries with primarily homosexual contact or injection drug use, and cervical cancer incidence (Table 2). Male circumcision was not associated with HSV-2, syphilis, nor, as expected, with the non-sexually-transmitted-disease prevalences of Hepatitis C, tuberculosis, or malaria. Among sub-Saharan African countries, HIV prevalence was 3.0% among countries with a high male circumcision prevalence and 16.5% among countries with a low male circumcision prevalence (p < 0.001). Among non-sub-Saharan African countries with primarily heterosexual HIV transmission, HIV prevalence was 0.09% among countries with a high male circumcision prevalence and 0.76% among countries with a low male circumcision prevalence (p < 0.001). Similarly,
the mean annual cervical cancer incidence was 20.5/ 100,000 women among countries with a high male circumcision prevalence and 35.0/100,000 women among countries with a low male circumcision prevalence (p < 0.001). Although there was no significant association between male circumcision and HSV-2 prevalence, the size and direction of the coefficient suggests that male circumcision could be associated with reduced HSV-2 prevalence given a larger sample size.
Religion and infectious diseases In univariate regression analyses, religion was also strongly associated with HIV and cervical cancer. Each percent increase of the population Muslim was associated with a 0.21/100,000 women (CI 0.15-0.28, p < 0.001) decrease in cervical cancer incidence, and a 1.25-fold (CI 1.16-1.35, p < 0.001) and 1.19-fold (CI 1.12-1.27, p < 0.001) decrease in adult HIV prevalence among sub-Saharan African and non-sub-Saharan African countries, respectively. Similarly, each percent increase of the population Christian was associated with a 0.26/100,000 women (CI 0.19-0.34, p < 0.001) increase in cervical can-
Page 4 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
Table 2: Male circumcision prevalence and selected infectious diseases among developing countries.
Univariate linear regression of male circumcision prevalence1 No. of countries HIV prevalence among sub-Saharan Africa (/100 adults)2 HIV prevalence among non-sub-Saharan African countries with primarily heterosexual HIV transmission (/100 adults)2 HIV prevalence among non-sub-Saharan African countries with primarily homosexual or injection drug use HIV transmission (/ 100 adults)2 Cervical cancer incidence (/100,000 women/year) Herpes Simplex Virus type-2 prevalence (/100 women) Tuberculosis prevalence (/100,000) Hepatitis C prevalence (/100 adults) Syphilis prevalence (/10,000 women) 38 29 33 117 23 110 75 43 Regression coefficient -0.90 -1.08 -1.03 -7.2 -6.1 25.9 0.20 51.7 R2* Countries with low (<20%) male circumcision prevalence No. of countries 8 11 25 51 10 48 37 20 Mean SD* Countries with high (>80%) male circumcision prevalence No. of countries 22 17 4 52 9 49 34 14 Mean SD*
0.51 0.51 0.29 0.18 0.08 0.01 0.003 0.0006
16.48 0.002 0.76 0.004 0.41 0.004 35.0 16.2 42.9 13.8 244 191 3.17 3.90 295 235
2.98 0.002 0.09 0.002 0.06 0.001 20.5 12.8 30.2 21.6 296 244 3.46 3.81 284 317
Malaria prevalence (/10,000)
94
-31.7
0.0007
31
385 887
31
331 596
SD standard deviation. * R2 values and mean values in bold type had p-values <0.001 and in italics type had p-values <0.05. R2 values and mean values not in bold or italics type had p-values >0.05. 1 Male circumcision prevalence was coded as 1 = low (<20%), 2 = intermediate (2080%), and 3 = high (>80%). 2 Regression analyses presented as natural log of HIV (prevalence/100,000 adults).
cer incidence, and a 1.32-fold (CI 1.20-1.45, p < 0.001) and 1.20-fold (CI 1.12-1.30, p < 0.001) increase in adult HIV prevalence among sub-Saharan African and non-subSaharan African countries, respectively.
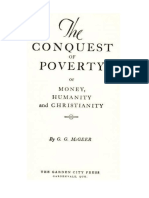
Male circumcision, religion, and infectious diseases Mean rates of cervical cancer incidence and HIV prevalence are presented among countries with low and high male circumcision prevalence in Figures 1, 2, 3, after separately stratifying countries into tertiles for percent Muslim and percent Christian. In nearly all religious tertile groups, mean cervical cancer incidence or HIV prevalence was lower among countries with a high male circumcision prevalence. Mean differences between high and low male circumcision groups were statistically significant for 7 of 14 (50%) tertile groups, and 2 additional tertile groups (14%) showed a borderline significance. When excluding each of the major religions in separate multivariate analyses, there were no meaningful changes in the associations between infectious diseases and male circumcision prevalence.
included in the model. In a multivariate model adjusted for 6 additional country-specific variables previously found to be associated with cervical cancer incidence [22], each categorical increase of male circumcision prevalence was highly associated with a 10.38/100,000 women (CI 4.94-15.82, p < 0.001) decrease in annual cervical cancer incidence. The 9 variables accounted for 59% of the variance in cervical cancer incidence among the 85 countries included in the model. Furthermore, male circumcision had a stronger association with cervical cancer incidence than all the other variables included in the model. Among sub-Saharan African countries, percent of the population Muslim and male circumcision, but not percent of the population Christian, remained independently associated with HIV prevalence (Table 4). After stratifying the countries by religious groups, each categorical increase of male circumcision prevalence was associated with a 1.84fold (CI 1.36-2.48, p < 0.001) decrease in adult HIV prevalence. In a multivariate model adjusted for 6 additional country-specific variables previously found to be associated with HIV prevalence [5], each categorical increase of male circumcision prevalence was associated with a 2.27fold (CI 1.51-3.42, p = 0.001) decrease in adult HIV prevalence. Among all non-sub-Saharan African countries, male circumcision remained independently associated with HIV prevalence among countries in regions with heterosexual contact as the primary mode of HIV transmission, but not among countries in regions with either homosexual contact or injection drug use as the primary mode of HIV transmission (Table 4). When stratifying the countries by
In a multivariate model, percent of the population Christian and male circumcision, but not percent of the population Muslim, remained independently associated with cervical cancer incidence (Table 3). After stratifying the countries by religious groups, each categorical increase of male circumcision prevalence was associated with a 3.65/ 100,000 women (CI 0.54-6.76, p = 0.02) decrease in annual cervical cancer incidence. These 3 measures (prevalence of male circumcision, percent Muslim, and percent Christian) accounted for 40% of the variance in cervical cancer incidence among the 105 developing countries
Page 5 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
45
Cervical Cancer Incidence (/100,000 women)
p = 0.0008 08 p = 0.041 41 p = 0.018 p = 0.053
40 0 35 30 25 20 15 10 5 0
p = 0.54 4 p = 0.45
Low MC High MC
Low est Muslim Tertile
Number of Countries:
Middle Muslim Tertile
Highest Muslim Tertile
Low est Cristian Tertile
Middle Christian Tertile
Highest Christian Tertile
30
14 14
7 36
9 24
7 20
35 8
Figure 1 the percent Muslim and Christian among 121by low (<20%) and high (>80%) male circumcision (MC) prevalence and tertiles of Cervical cancer incidence (/100,000 women) developing countries Cervical cancer incidence (/100,000 women) by low (<20%) and high (>80%) male circumcision (MC) prevalence and tertiles of the percent Muslim and Christian among 121 developing countries. religious groups among countries with primarily heterosexual HIV transmission, each categorical increase of male circumcision prevalence was associated with a 8.94-fold (95% CI 4.30-18.60) decrease in adult HIV prevalence. In a multivariate model adjusted for 6 additional countryspecific variables [5], each categorical increase of male circumcision prevalence was associated with a 4.94-fold (95% CI 2.29-10.65, p = 0.001) decrease in adult HIV prevalence. In a separate multivariate model, after stratifying the countries by religious groups among countries with primarily homosexual contact or injection drug use HIV transmission, male circumcision was not significantly associated with HIV prevalence (p = 0.35). When adjusting the multivariate model for the 6 additional countryspecific variables [5], male circumcision prevalence was not significantly associated with HIV prevalence (p = 0.70). mitted by non-sexual routes. In general, more male circumcision was strongly associated with lower cervical cancer rates and fewer HIV cases, independent of religion. Furthermore, male circumcision was independently associated with HIV among countries with primarily heterosexual HIV transmission, and not among countries with primarily homosexual or injection drug use HIV transmission. These findings all suggest that male circumcision is a true protective factor that reduces the sexual transmission of HIV and possibly HPV, independent of Muslim and Christian religions. An ecologic study of this type has limitations, as we have previously acknowledged [5,22]. In brief, ecological analyses cannot measure correlates of risk at the individuallevel. Second, the temporal sequence of events in individuals is undetermined. Since the approximate age at circumcision varies by country, the results could be affected if a significant proportion delayed male circumcision until after initiation of sexual activity. Third, the validity of country-level data undoubtedly varies, and some data, such as HSV-2 prevalence, were not available for many countries. Although mean HSV-2 prevalence was lower among countries with more male circumcision, the limited number of countries with HSV-2 data (23 countries) gave relatively low power for examining the significance of this association. Fourth, and perhaps most importantly,
Discussion
This ecological study of 118 developing countries expands results from our previous analyses [5,22] by elucidating patterns and associations between male circumcision, religion, and infectious diseases, particularly HIV. Male circumcision, which is routinely practiced in the Middle East, northern and western Africa, and western Asia, was associated with lower rates of certain STIs, HIV and cervical cancer (a proxy for HPV), but not with infections trans-
Page 6 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
12
p = 0.011 11 p = 0.12 p = 0.033 p = 0.027
HIV Prevalence (ln/100,000 adults)
10
8 Low MC High MC 4
0 Low est Muslim Tertile
Number of Countries:
Middle Muslim Tertile
Highest Muslim Tertile
Low est Cristian Tertile
Middle Christian Tertile
Highest Christian Tertile
4 11
2 13
6 5
Figure 2 Muslim and Christian among 38 by low (<20%) and countries with primarily heterosexual HIV transmission the percent HIV prevalence (/100,000 adults) sub-Saharan Africanhigh (>80%) male circumcision (MC) prevalence and tertiles of Natural log Natural log HIV prevalence (/100,000 adults) by low (<20%) and high (>80%) male circumcision (MC) prevalence and tertiles of the percent Muslim and Christian among 38 sub-Saharan African countries with primarily heterosexual HIV transmission.
statistics on the distribution and variation within countries were not complete. Some countries, such as Kenya, have widely varying regional prevalences of male circumcision and HIV [32]. For example, western Kenya, where less than 20% of males are circumcised, has a much higher HIV prevalence than regions of the country where nearly all men are circumcised [3,32]. The 2003 Kenya survey also found uncircumcised males had over three-fold higher HIV prevalence as compared to circumcised males, and HIV prevalence in circumcised men was nearly identical among the major religious groups (2.6% among Catholics, 3.0% in Protestant/other Christians, and 2.9% in Muslims) [32]. Finally, not all population-level measures that may impact infectious disease transmission, such as patterns of risk behaviors, condom availability and utilization, and injection drug use, were included in this analysis. Despite these limitations, findings from this ecological analysis support a biological relationship between male circumcision and certain STIs. Previous studies, including a recent Cochrane review [16], have also found male circumcision to be associated with a reduced risk of HPV detection in men [14], cervical cancer in female partners [13], and HIV infection [3,11,12,15,17], while associations between male circumcision and HSV-2 and gonorrhea are less clear [15,19,43].
However, these studies were generally conducted among geographically-limited populations and many were unable to adequately control for religion. By comparison, our study described the global distribution of male circumcision prevalence, examined a large number of geographically-diverse countries and several infectious diseases, separately analyzed countries by primarily heterosexual and non-heterosexual transmission of HIV, and included relatively complete and recent surveillance data. Our study supports results of other studies by demonstrating independent associations of male circumcision with reduced cervical cancer rates and HIV cases, after stratifying the countries for Muslim and Christian religions, among a large sample of developing countries. Others have described biologically plausible mechanisms by which male circumcision may reduce the transmission of certain STIs [18,19,44,45]. First, circumcised males may have less difficulty maintaining penile hygiene, which may reduce the acquisition of STIs by decreasing inflammation and the carriage time of pathogens in the foreskin [19,45]. Secondly, the non-keratinized epidermis of the prepuce in uncircumcised males may provide an easier portal of entry to STIs [19,44,45]. Third, the inner mucosal surface of the prepuce, which has a high density of HIV target cells (CD4+ T-cells, Langerhans cells, macro-
Page 7 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
p = 0.008
HIV Prevalence (ln/100,000 adults)
p = 0.26
7 6 5
p = 0.08 p = N/A
p = N/A
4 3 2 1 0 Lowest Muslim Middle Muslim Highest Lowest Middle Tertile Tertile Muslim Tertile Cristian Tertile Christian Tertile Highest Christian Tertile
Low MC High MC
Number of Countries:
2 1
4 16
3 10
1 5
Figure 3 Muslim and Christian among 29 by low (<20%) and high countries with primarily (MC) prevalence transmission the percent HIV prevalence (/100,000 adults) non-sub-Saharan African(>80%) male circumcisionheterosexual HIV and tertiles of Natural log Natural log HIV prevalence (/100,000 adults) by low (<20%) and high (>80%) male circumcision (MC) prevalence and tertiles of the percent Muslim and Christian among 29 non-sub-Saharan African countries with primarily heterosexual HIV transmission.
phages), has been shown to become more easily infected with HIV as compared to outer foreskin tissue [45]. Given these biological differences, it is entirely plausible that uncircumcised males are at a greater risk of acquiring some STIs, and of transmitting them to their sexual partners [12]. According to UNAIDS, heterosexual transmission was the primary mode of HIV transmission in Africa, the Middle East, the Caribbean, and South and South-East Asia, and homosexual transmission was the primary mode of HIV
transmission in Latin America [37]. In our analysis, male circumcision was strongly associated with HIV among developing countries with heterosexual contact as the primary mode of HIV transmission, and not among developing countries whose primary mode of HIV transmission was not heterosexual contact (Eastern Europe, Central and Eastern Asia, Latin America, and the Pacific). These results further support the biological role of male circumcision as a protective factor in HIV transmission. Furthermore, the fact that HIV prevalence in many predominantly Christian countries that practice male circumcision, such as the
Table 3: Multivariate linear regression models of cervical cancer incidence (/100,000 women/year) among developing countries.
No. of countries Unadjusted regression model Percent of population Muslim Percent of population Christian Male circumcision prevalence1 Adjusted regression model2 Percent of population Muslim Percent of population Christian Male circumcision prevalence1
1 Male
coefficient
p-value
R2 0.40
105 -0.010 0.21 -3.65 85 0.083 0.13 -10.38 0.25 0.017 <0.001 0.84 <0.001 0.022
0.59
2 Model
circumcision prevalence was coded as 1 = low (<20%), 2 = intermediate (2080%), and 3 = high (>80%). adjusted by country-specific measures including number of doctors per 100,000 people, percent of children immunized for measles, female disability-adjusted life expectancy in years, percent of female adult illiteracy rate, percent of infants with low birth weight, and major geographic region.
Page 8 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
Table 4: Multivariate linear regression models of HIV prevalence (/100,000 adults) among developing countries.1
Sub-Saharan African countries with heterosexual contact as primary mode of HIV transmission No. of countries Unadjusted regression model Percent of population Muslim Percent of population Christian Male circumcision prevalence2 Adjusted regression model3 Percent of population Muslim Percent of population Christian Male circumcision prevalence2
1 Analyses 2 Male
Non-Sub-Saharan African countries with heterosexual contact as primary mode of HIV transmission No. of countries 24 0.031 0.021 -2.19 0.02 0.04 <0.001 0.72 0.014 0.0011 -1.60 0.19 0.94 0.001 Regression coefficient p-value R2
Non-Sub-Saharan African countrieswith homosexual contact or injection-drug use as primary mode of HIV transmission No. of countries 32 0.021 0.017 -1.26 23 -0.036 0.015 0.47 0.26 0.15 0.70 0.51 0.003 0.35 0.73 Regression coefficient p-value R2
Regression coefficient
p-value
R2
35 -0.013 0.0015 -0.61 27 -0.011 -0.0044 -0.82 0.026 0.48 0.001 0.023 0.84 <0.001
0.68
0.70
0.49
0.85
22
conducted with natural log of HIV seroprevalence. circumcision prevalence was coded as 1 = low (<20%), 2 = intermediate (2080%), and 3 = high (>80%). 3 Model adjusted by country-specific measures including years since HIV was first reported, major geographical region, percent of population younger than age 25, percent of female adult illiteracy rate, percent of children fully immunized for diphtheria, tetanus, and pertussis, and number of doctors per 100,000 people.
Philippines, Benin, Ghana, Equatorial Guinea, and Gabon, is similarly low as in predominantly Muslim countries in the same regions, suggests that the biological effect of male circumcision may be at least as important as religion in determining HIV prevalence [24].
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
PKD, DTH, JPH, and RCB designed the study. PKD, DTH, and RCB collected and analyzed data. PKD, DTH, JPH, JDK, and RCB interpreted the results. PKD primarily wrote the manuscript. DTH, JPH, JDK, and RCB provided valuable insight for revising the manuscript. All authors read and approved the final manuscript.
Conclusion
This study demonstrates that male circumcision was strongly associated with lower cervical cancer rates and fewer HIV cases among countries with heterosexual contact as the primary mode of HIV transmission, independent of religion. One randomized controlled trial has demonstrated that male circumcision is highly protective of HIV acquisition [21]. Therefore, while HIV and cervical cancer are impacted by a complex set of biological, social, and public health influences, male circumcision appears to play a prominent role in decreasing transmission of certain STIs. Although male circumcision must not substitute for other HIV and STI prevention strategies [46], the international public health and medical community should consider the implications and practicalities of integrating safe, voluntary male circumcision services with existing HIV prevention programs, particularly in countries with low prevalence of male circumcision and high prevalence of sexually-transmitted HIV.
Acknowledgements
Supported by the University of Washington Center for AIDS Research Grant AI 27757 and University of Washington STD Cooperative Research Center Grant AI 31448. The National Institutes of Health had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for publication. The authors wish to thank David Wilson, Antonio de Moya and Jeff Marck for reviewing classification of countries by male circumcision prevalence, King Holmes and Beth Weaver-Green for reviewing drafts of the manuscript, and Mary Fielder and Ron Nelson for assistance with manuscript preparations.
References
1. 2. Caldwell JC, Caldwell P: The African AIDS epidemic. Sci Am 1996, 274:62-3. Carael M, Buv A, Awusabo-Asare K: The making of HIV epidemics: What are the driving forces? AIDS 1997, 2(Suppl):185-205. Auvert B, Buv A, Ferry B, Carael M, Morison L, Lagarde E, Robinson NJ, Kahindo M, Chege J, Rutenberg N, Musonda R, Laourou M, Akam E, Study Group on the Heterogeneity of HIV Epidemics in African Cities: Ecological and individual level analysis of risk factors for HIV infection in four urban populations in sub-Saharan Africa with different levels of HIV infection. AIDS 2001, 15(Suppl 4):S15-S30. Auvert B, Ferry B: Modeling the spread of HIV infection in four cities of sub-Saharan Africa [abstract]. Presented at XIV International AIDS Conference, 2002; Barcelona. Drain PK, Smith JS, Hughes JP, Halperin DT, Holmes KK: Correlates of national HIV seroprevalence. An ecological analysis of 122
Abbreviations
HIV human immunodeficiency virus; HSV-2 herpes simplex virus type-2; STIs sexually-transmitted infections; UNDP United Nations Development Programme; UNAIDS The Joint United Nations Programme on HIV/ AIDS; HPV human papillomavirus;
3.
4. 5.
Page 9 of 10
(page number not for citation purposes)
BMC Infectious Diseases 2006, 6:172
http://www.biomedcentral.com/1471-2334/6/172
6. 7.
8.
9. 10. 11.
12.
13.
14.
15.
16.
17. 18.
19. 20. 21.
22. 23. 24. 25. 26.
developing countries. J Acquir Immune Defic Syndr 2004, 35:407-420. Bongaarts J, Reining P, Way P, Conant F: The relationship between male circumcision and HIV infection in African populations. AIDS 1989, 3:373-377. Cameron DW, Simonsen JN, D'Costa LJ, Ronald AR, Maitha GM, Gakinya MN, Cheang M, Ndinya-Achola JO, Piot P, Brunham RC: Female to male transmission of human immunodeficiency virus type 1: risk factors for seroconversion in men. Lancet 1989, 2:403-407. Moses S, Bradley J, Nagelkerke N, Ronald AR, Ndinya-Achola JP, Plummer FA: Geographical patterns of male circumcision practices in Africa: association with HIV prevalence. Int J Epidem 1990, 19:693-697. Gray PB: HIV and Islam: is HIV prevalence lower among Muslims? Soc Sci & Med 2004, 58:1751-1756. Halperin DT, Bailey RC: Male circumcision and HIV infection: 10 years and counting. Lancet 1999, 354:1813-1815. Lavreys L, Rakwar JP, Thompson ML, Jackson DJ, Mandaliya K, Chohan BH, Bwayo JJ, Ndinya-Achola JO, Kreiss JK: Effect of circumcision on incidence of HIV and other STDs: a prospective cohort study of truck company employees in Kenya. J Infect Dis 1999, 180:330-336. Gray RH, Kiwanuka N, Quinn TC, Sewankambo NK, Serwadda D, Mangen FW, Lutalo T, Nalugoda F, Kelly R, Meehan M, Chen MZ, Li C, Wawer MJ, for the Rakai Project Team: Male circumcision and HIV acquisition and transmission: cohort studies in Rakai, Uganda. AIDS 2000, 14:2371-2381. Castellsague X, Bosch FX, Munoz N, Meijer CJ, Shah KV, de Sanjose S, Eluf-Neto J, Ngelangel CA, Chichareon S, Smith JS, Herrero R, Moreno V, Franceschi S, International Agency for Research on Cancer Multicenter Cervical Cancer Study Group: Male circumcision, penile Human Papillomavirus infection, and cervical cancer in female partners. N Engl J Med 2002, 346:1105-1112. Baldwin SB, Wallace DR, Papenfuss MR, Abrahamsen M, Vaught LC, Giuliano AR: Condom use and other factors affecting penile Human Papillomavirus detection in men attending a sexually transmitted disease clinic. Sex Trans Dis 2004, 31:601-607. Reynolds SJ, Shepherd ME, Risbud AR, Gangakhedkar RR, Brookmeyer RS, Divekar AD, Mehendale SM, Bollinger RC: Male circumcision and risk of HIV-1 and other sexually transmitted infections in India. Lancet 2004, 363:1039-1040. Siegfried N, Muller M, Volmink J, Deeks J, Egger M, Low N, Weiss H, Walker S, Williamson P: Male circumcision for prevention of heterosexual acquisition of HIV in men. Cochrane Database Syst Rev 2003, 3:CD003362. Weiss HA, Quigley MA, Hayes RJ: Male circumcision and risk of HIV infection in sub-Saharan Africa: a systematic review and meta-analysis. AIDS 2000, 14:2361-2370. Moses S, Plummer FA, Bradley JE, Ndinya-Achola JO, Nagelkerke NJ, Ronald AR: The association between lack of male circumcision and risk for HIV infection: a review of the epidemiological data. Sex Trans Dis 1994, 21:201-210. Bailey RC, Plummer FA, Moses S: Male circumcision and HIV prevention: current knowledge and future research directions. Lancet Infect Dis 2001, 1:223-231. Carael M, Cleland J, Deheneffe JC, Ferry B, Ingham R: Sexual behaviour in developing countries: implications for HIV control. AIDS 1995, 9:1171-1175. Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A: Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: The ANRS 1265 trial. PLoS Med 29:e298. Drain PK, Holmes KK, Hughes JP, Koutsky LA: Determinants of cervical cancer rates in developing countries. Int J Cancer 2002, 100:199-205. United Nations Development Programme: Human Development Report 2004 New York: Oxford University Press; 2004. Joint United Nations Programme on HIV/AIDS: Report on the Global HIV/AIDS Epidemic 2004 Geneva: UNAIDS; 2004. Smith JS, Robinson J: Herpes simplex virus infections: a review of seroprevalence worldwide. J Infect Dis 2002, 186(Suppl 1):S3-28. Ferlay J, Bray F, Pisani P, Parkin DM: GLOBOCAN 2000: Cancer Incidence, Mortality, and Prevalence Worldwide, Version 1.0 2001 [http://
27. 28. 29. 30. 31. 32.
33. 34. 35. 36. 37. 38. 39. 40.
41. 42. 43. 44. 45.
46.
www-dep.iarc.fr]. International Agency for Research on Cancer CancerBase No. 5 Lyon, IARCPress George Schmid, World Health Organization: Personal communication on June 4. 2004. World Health Organization: Hepatitis C Global Prevalence (update). Weekly Epidemiol Rec 1999, 49:425-427. Bailey RC, Neema S, Othieno R: Sexual behaviors and other HIV risk factors in circumcised and uncircumcised men in Uganda. J Acquir Immune Defic Syndr 1999, 22:294-301. Kebaabetswe P, Lockman S, Mogwe S, Mandevu R, Thior I, Essex M, Shapiro RL: Male circumcision: an acceptable strategy for HIV prevention in Botswana. Sex Transm Infect 2003, 79:214-219. Addis Ababa University, Family Health International: Behavioral Surveillance Survey (BSS), Ethiopia 2002 Addis Ababa, Ethiopia: Addis Ababa University, Family Health International; 2003. Kenya Bureau of Statistics/Ministry of Health/Medical Research Institute/Center for Disease Control Macro International: Kenya Demographic and Health Survey, 2003 2003 [http://www.measuredhs.com/ pubs/pdf/FR151/13Chapter13.pdf]. Calverton, Maryland: Macro International World Health Organization/Global Program on AIDS: 1989 Uganda Survey Geneva: World Health Organization; 1989. Macro International: Demographic and Health Surveys data base 2004 [http://www.measuredhs.com]. Calverton, Maryland: Marco International Measure Evaluation: Central Statistical Office/Ministry of Health, Zambia. Zambia Sexual Behavior Survey 2003 [http:// www.cpc.unc.edu/measure/publications/pdf/tr-04-19.pdf]. United Nations Population Division: World Population Prospects: The 2000 Revision New York: United Nations; 2001. Joint United Nations Programme on HIV/AIDS: HIV/AIDS Epidemic Update 2002 Geneva: UNAIDS; 2002. United States Central Intelligence Agency: The World Factbook 2001 2000 [http://www.odci.gov/cia/publications/factbook]. Washington DC: US Government Printing Office StataCorp: Stata Statistical Software: Release 8.0 College Station, Texas: Stata Corporation; 2004. Caldwell JC, Caldwell P, Orubuloye IO: The family and sexual networking in sub-Saharan Africa: historical regional differentials and present-day implications. Population Studies 1992, 46:385-410. Carael M: Sexual behaviour. In Sexual Behaviour and AIDS in the Developing World Edited by: Cleland J and Ferry B. London: Taylor & Francis; 1995:75-123. Halperin DT, Epstein H: Concurrent sexual partnerships help to explain Africa's high HIV prevalence: implications for prevention. Lancet 2004, 363:4-6. Weiss HA, Thomas SL, Munabi SK, Hayes RJ: Male circumcision and risk of syphilis, chancroid and genital herpes: a systematic review and meta-analysis. STI Online 2006, 82:101-110. Szabo R, Short RV: How does male circumcision protect against HIV infection? BMJ 2000, 320:1592-1594. Patterson BK, Landay A, Siegel JN, Flener Z, Pessis D, Chaviano A, Bailey RC: Susceptibility to human immunodeficiency virus-1 infection of human foreskin and cervical tissue grown in explant culture. Amer J Pathology 2002, 16:867-873. Halperin DT, Steiner MJ, Cassell MM, Green EC, Hearst N, Kirby D, Gayle HD, Cates W: The time has come for common ground on preventing sexual transmission of HIV. Lancet 2004, 364:1913-1915.
Pre-publication history
The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2334/6/172/pre pub
Page 10 of 10
(page number not for citation purposes)
You might also like
- Eustace Mullins - The World Order - Rare and Great BookDocument282 pagesEustace Mullins - The World Order - Rare and Great BookTerell A Banks80% (5)
- Ezra Pound Speaking - Radio Speeches of World War II - Edited by Leonard W. Doob, Greenwood Press, 1978Document205 pagesEzra Pound Speaking - Radio Speeches of World War II - Edited by Leonard W. Doob, Greenwood Press, 1978Domenico BevilacquaNo ratings yet
- Wells Fargo StatementDocument4 pagesWells Fargo Statementandy0% (1)
- Safety Moment Manual LiftingDocument1 pageSafety Moment Manual LiftingEvert W. VanderBerg100% (1)
- FraudDocument77 pagesFraudTan Siew Li100% (2)
- Harmonizing A MelodyDocument6 pagesHarmonizing A MelodyJane100% (1)
- Ben Franklin and Paper Money EconomyDocument12 pagesBen Franklin and Paper Money EconomyPaul Jensen100% (1)
- Follow The Money, by Kirk MacKenzieDocument31 pagesFollow The Money, by Kirk MacKenzieDomenico BevilacquaNo ratings yet
- Money of The American Colonies and Confederation, by Philip Mossman, American Numismatic Society, New York, 1993Document338 pagesMoney of The American Colonies and Confederation, by Philip Mossman, American Numismatic Society, New York, 1993Domenico Bevilacqua100% (1)
- Strategies for Awareness & Prevention of Hiv/Aids Among African-Americans: A Hand BookFrom EverandStrategies for Awareness & Prevention of Hiv/Aids Among African-Americans: A Hand BookNo ratings yet
- FS2 Learning Experience 1Document11 pagesFS2 Learning Experience 1Jona May BastidaNo ratings yet
- Sigmund Freud QuotesDocument7 pagesSigmund Freud Quotesarbeta100% (2)
- Factors Affecting Job Satisfaction of EngineersDocument35 pagesFactors Affecting Job Satisfaction of Engineerslingg8850% (2)
- Artikel-Hiv-Ayu NingrumDocument7 pagesArtikel-Hiv-Ayu NingrumAyu NingrumNo ratings yet
- National HIV Testing Day - June 27, 2010 Expanded HIV Testing and Trends in Diagnoses of HIV Infection - District of Columbia, 2004-2008Document32 pagesNational HIV Testing Day - June 27, 2010 Expanded HIV Testing and Trends in Diagnoses of HIV Infection - District of Columbia, 2004-2008worksheetbookNo ratings yet
- Journal Pmed 1003861Document18 pagesJournal Pmed 1003861Anastasi MokgobuNo ratings yet
- EF08L44Document25 pagesEF08L44vinfinityindiaNo ratings yet
- Stis in SwazilandDocument12 pagesStis in SwazilandMuhammad FansyuriNo ratings yet
- Five-Year Trends in Epidemiology and Prevention of Mother-To-Child HIV Transmission, St. Petersburg, Russia: Results From Perinatal HIV SurveillanceDocument11 pagesFive-Year Trends in Epidemiology and Prevention of Mother-To-Child HIV Transmission, St. Petersburg, Russia: Results From Perinatal HIV SurveillanceManuela Martín-Bejarano GarcíaNo ratings yet
- HIV Transmission and Prevention: Mother-to-Child (Perinatal)Document5 pagesHIV Transmission and Prevention: Mother-to-Child (Perinatal)Wahyu Wijasena AdhiNo ratings yet
- Rates and barriers of HIV status disclosure among women in developing countriesDocument9 pagesRates and barriers of HIV status disclosure among women in developing countriesTinkhaniMbichilaNo ratings yet
- HIV and Islam Is HIV Prevalence Lower Am PDFDocument6 pagesHIV and Islam Is HIV Prevalence Lower Am PDFPriyo DjatmikoNo ratings yet
- Defining Rights-Based Indicators For HIV Epidemic TransitionDocument7 pagesDefining Rights-Based Indicators For HIV Epidemic TransitionDanylo VianaNo ratings yet
- MM 5904Document28 pagesMM 5904Raul Hernandez HernandezNo ratings yet
- Sexually Transmitted Diseases Among American Youth: Incidence and Prevalence Estimates, 2000Document5 pagesSexually Transmitted Diseases Among American Youth: Incidence and Prevalence Estimates, 2000Amalia nurlailyNo ratings yet
- The Socio-Economic Determinants of HIV/AIDS Infection Rates in Lesotho, Malawi, Swaziland and ZimbabweDocument22 pagesThe Socio-Economic Determinants of HIV/AIDS Infection Rates in Lesotho, Malawi, Swaziland and Zimbabweecobalas7No ratings yet
- Ijerph 19 09331 v2Document13 pagesIjerph 19 09331 v2Aklilu FelekeNo ratings yet
- Among Youth: Hiv/AidsDocument5 pagesAmong Youth: Hiv/AidsShahnaz RizkaNo ratings yet
- The Global Epidemiology of Bacterial Vaginosis A Systematic ReviewDocument19 pagesThe Global Epidemiology of Bacterial Vaginosis A Systematic ReviewcheracapNo ratings yet
- Sexually Transmitted Diseases Among Adolescents in Developed CountriesDocument16 pagesSexually Transmitted Diseases Among Adolescents in Developed CountriesJudith AmarteyNo ratings yet
- HIV Infection - Risk Factors and Prevention Strategies - UpToDateDocument23 pagesHIV Infection - Risk Factors and Prevention Strategies - UpToDateDaniel EspinozaNo ratings yet
- Vital Signs: HIV Infection, Testing, and Risk Behaviors Among Youths - United StatesDocument6 pagesVital Signs: HIV Infection, Testing, and Risk Behaviors Among Youths - United Statessmf 4LAKidsNo ratings yet
- Djimeu Published Replication PlanDocument17 pagesDjimeu Published Replication PlanVishalvishaldograNo ratings yet
- Artículo Juanito UTDDocument21 pagesArtículo Juanito UTDJulián DuránNo ratings yet
- CDC FACT SHEET: Reported STDs in The United States - 2012 National Data For Chlamydia, Gonorrhea, and SyphilisDocument3 pagesCDC FACT SHEET: Reported STDs in The United States - 2012 National Data For Chlamydia, Gonorrhea, and Syphilistherepubliq.comNo ratings yet
- Knowledge and Attitude of HIV/AIDS Among Women in Nigeria: A Cross-Sectional StudyDocument7 pagesKnowledge and Attitude of HIV/AIDS Among Women in Nigeria: A Cross-Sectional StudyDele ValentineNo ratings yet
- Best Practice Research Paper FinalDocument11 pagesBest Practice Research Paper Finalapi-354544160No ratings yet
- Interventions To Prevent Sexually Transmitted Infections, Including HIV InfectionDocument15 pagesInterventions To Prevent Sexually Transmitted Infections, Including HIV Infectionursula_ursulaNo ratings yet
- HIV Associated High-Risk HPV Infection Among Nigerian Women: Researcharticle Open AccessDocument6 pagesHIV Associated High-Risk HPV Infection Among Nigerian Women: Researcharticle Open AccessMay MaghdalenaNo ratings yet
- HIV and AIDS where is the epidemic goingDocument9 pagesHIV and AIDS where is the epidemic going1w3r5y7i9p10qpNo ratings yet
- Su7301a1 HDocument8 pagesSu7301a1 HSAFWA BATOOL NAQVINo ratings yet
- Male Circumcision and Risk of HIV Infection in Sub-Saharan Africa: A Systematic Review and Meta-AnalysisDocument10 pagesMale Circumcision and Risk of HIV Infection in Sub-Saharan Africa: A Systematic Review and Meta-AnalysisJpt YapNo ratings yet
- Epidemiology, Transmission, and Prevention of Hepatitis B Virus Infection - UpToDateDocument20 pagesEpidemiology, Transmission, and Prevention of Hepatitis B Virus Infection - UpToDatehochanh199xNo ratings yet
- According To CDC: Biologic PlausibilityDocument7 pagesAccording To CDC: Biologic PlausibilityJpt YapNo ratings yet
- CommunityViralLoadinHIV PDFDocument9 pagesCommunityViralLoadinHIV PDFIsaias PrestesNo ratings yet
- Navigating Disclosure Obstacles Encountered by Individuals With HIV at Kakomo Healing Centre IV in Kabale DistrictDocument15 pagesNavigating Disclosure Obstacles Encountered by Individuals With HIV at Kakomo Healing Centre IV in Kabale DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Using HPV Prevalence To Predict Cervical Cancer IncidenceDocument6 pagesUsing HPV Prevalence To Predict Cervical Cancer Incidencenyoman2No ratings yet
- Galvin Role of StisDocument10 pagesGalvin Role of StisMatin Ahmad KhanNo ratings yet
- MC For HIV Prevention Fact Sheet - 508Document3 pagesMC For HIV Prevention Fact Sheet - 508Zunga MwaangaNo ratings yet
- Sande's HIV - AIDS Medicine (PDFDrive)Document562 pagesSande's HIV - AIDS Medicine (PDFDrive)angel muñozNo ratings yet
- Setting Research Priorities For Adolescent Sexual and Reproductive Health in Low - and Middle-Income CountriesDocument9 pagesSetting Research Priorities For Adolescent Sexual and Reproductive Health in Low - and Middle-Income CountriesArio PalandengNo ratings yet
- The Epidemiology of AIDS: Distribution, Determinants and ControlDocument44 pagesThe Epidemiology of AIDS: Distribution, Determinants and ControlKelssey Pierre-louisNo ratings yet
- Ensuring Access To Sexually Transmitted Infection Care For AllDocument13 pagesEnsuring Access To Sexually Transmitted Infection Care For AllCenter for American ProgressNo ratings yet
- Community Assessment of ChlamydiaDocument23 pagesCommunity Assessment of Chlamydiaapi-262409636100% (1)
- Prevention Challenges and SolutionsDocument4 pagesPrevention Challenges and SolutionsAnonymous nPHRSvb2WNo ratings yet
- Hiv and Aids AssDocument9 pagesHiv and Aids AssquarozNo ratings yet
- STD Screening and PreventionDocument12 pagesSTD Screening and PreventionjordyeeNo ratings yet
- HIV Rates in Low Income CommunitiesDocument7 pagesHIV Rates in Low Income CommunitiesAnungo KaveleNo ratings yet
- Level of Awareness on HIV/AIDS among Adolescent MSMDocument19 pagesLevel of Awareness on HIV/AIDS among Adolescent MSMFritz MaandigNo ratings yet
- Group 1 HIVDocument22 pagesGroup 1 HIVmameandarg7No ratings yet
- Diare PDFDocument10 pagesDiare PDFMoonika TodinganNo ratings yet
- Epidemiology of HIV and AIDS Among Adolescents 169Document10 pagesEpidemiology of HIV and AIDS Among Adolescents 169Genevieve Caecilia Linda KNo ratings yet
- Epidemiology, Transmission, and Prevention of Hepatitis B Virus InfectionDocument20 pagesEpidemiology, Transmission, and Prevention of Hepatitis B Virus Infectionmayteveronica1000No ratings yet
- How HIV Is DetectedDocument12 pagesHow HIV Is DetectedTaranisaNo ratings yet
- Research Paper On Aids in AmericaDocument6 pagesResearch Paper On Aids in Americajssoulznd100% (1)
- HIV Infection Epidemiology, Pathogenesis, Treatment, and PreventionDocument14 pagesHIV Infection Epidemiology, Pathogenesis, Treatment, and PreventionandresgarciafNo ratings yet
- Anogenital Anatomy and Sexual HIV SpreadDocument18 pagesAnogenital Anatomy and Sexual HIV SpreadBastian FischerNo ratings yet
- Journal Hiv - Aids: Disusun Untuk Memenuhi Tugas Mata Kuliah Keperawatan HIV-AIDSDocument13 pagesJournal Hiv - Aids: Disusun Untuk Memenuhi Tugas Mata Kuliah Keperawatan HIV-AIDSarya andika saputraNo ratings yet
- HIV Epidemiology Among Female Sex Workers and Their Clients in The Middle East and North Africa: Systematic Review, Meta-Analyses, and Meta-RegressionsDocument30 pagesHIV Epidemiology Among Female Sex Workers and Their Clients in The Middle East and North Africa: Systematic Review, Meta-Analyses, and Meta-RegressionsLuís MiguelNo ratings yet
- Final AssignmentDocument6 pagesFinal Assignmentapi-450946351No ratings yet
- Prevalence of Sexually Transmitted Infections and Associated Factors Among The University StudentsDocument11 pagesPrevalence of Sexually Transmitted Infections and Associated Factors Among The University Studentsijmb333No ratings yet
- The Autobiography of Martin Van Buren, Government Printing Office, Washington, 1920Document820 pagesThe Autobiography of Martin Van Buren, Government Printing Office, Washington, 1920Domenico BevilacquaNo ratings yet
- The Conquest of PovertyDocument174 pagesThe Conquest of PovertyDomenico BevilacquaNo ratings yet
- History: MoneyDocument68 pagesHistory: MoneyDomenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1976Document83 pagesCar Care Guide - Popular Mechanics - May 1976Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1990Document40 pagesCar Care Guide - Popular Mechanics - May 1990Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1978Document93 pagesCar Care Guide - Popular Mechanics - May 1978Domenico BevilacquaNo ratings yet
- SeigniorageDocument50 pagesSeigniorageDomenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1988Document52 pagesCar Care Guide - Popular Mechanics - May 1988Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1984Document60 pagesCar Care Guide - Popular Mechanics - May 1984Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1986Document82 pagesCar Care Guide - Popular Mechanics - May 1986Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1985Document63 pagesCar Care Guide - Popular Mechanics - May 1985Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - Oct 1979Document40 pagesCar Care Guide - Popular Mechanics - Oct 1979Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1987Document61 pagesCar Care Guide - Popular Mechanics - May 1987Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1982Document71 pagesCar Care Guide - Popular Mechanics - May 1982Domenico Bevilacqua100% (1)
- Car Care Guide - Popular Mechanics - May 1983Document71 pagesCar Care Guide - Popular Mechanics - May 1983Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - Oct 1983Document31 pagesCar Care Guide - Popular Mechanics - Oct 1983Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1980Document95 pagesCar Care Guide - Popular Mechanics - May 1980Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1979Document99 pagesCar Care Guide - Popular Mechanics - May 1979Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - Oct 1982Document54 pagesCar Care Guide - Popular Mechanics - Oct 1982Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - Oct 1981Document52 pagesCar Care Guide - Popular Mechanics - Oct 1981Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - Oct 1980Document62 pagesCar Care Guide - Popular Mechanics - Oct 1980Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1981Document89 pagesCar Care Guide - Popular Mechanics - May 1981Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1977Document108 pagesCar Care Guide - Popular Mechanics - May 1977Domenico Bevilacqua100% (1)
- Car Care Guide - Popular Mechanics - May 1974Document92 pagesCar Care Guide - Popular Mechanics - May 1974Domenico BevilacquaNo ratings yet
- Car Care Guide - Popular Mechanics - May 1975Document72 pagesCar Care Guide - Popular Mechanics - May 1975Domenico BevilacquaNo ratings yet
- Unit 9 What Does APES Say?Document17 pagesUnit 9 What Does APES Say?johnosborneNo ratings yet
- Lab 5: Conditional probability and contingency tablesDocument6 pagesLab 5: Conditional probability and contingency tablesmlunguNo ratings yet
- Brochure - Coming To Work in The Netherlands (2022)Document16 pagesBrochure - Coming To Work in The Netherlands (2022)Tshifhiwa MathivhaNo ratings yet
- Computer Conferencing and Content AnalysisDocument22 pagesComputer Conferencing and Content AnalysisCarina Mariel GrisolíaNo ratings yet
- History Project Reforms of Lord William Bentinck: Submitted By: Under The Guidelines ofDocument22 pagesHistory Project Reforms of Lord William Bentinck: Submitted By: Under The Guidelines ofshavyNo ratings yet
- 100 Bedded Hospital at Jadcherla: Load CalculationsDocument3 pages100 Bedded Hospital at Jadcherla: Load Calculationskiran raghukiranNo ratings yet
- Business Planning Process: Chapter-Four Operations Planning and ControlDocument12 pagesBusiness Planning Process: Chapter-Four Operations Planning and ControlGemechis BussaNo ratings yet
- Lesson 6 (New) Medication History InterviewDocument6 pagesLesson 6 (New) Medication History InterviewVincent Joshua TriboNo ratings yet
- Cover Me: Music By: B. Keith Haygood Arranged By: BKH Lyrics By: Based On Exodus 33Document8 pagesCover Me: Music By: B. Keith Haygood Arranged By: BKH Lyrics By: Based On Exodus 33api-66052920No ratings yet
- BMW E9x Code ListDocument2 pagesBMW E9x Code ListTomasz FlisNo ratings yet
- Discover books online with Google Book SearchDocument278 pagesDiscover books online with Google Book Searchazizan4545No ratings yet
- Understanding Learning Theories and Knowledge AcquisitionDocument38 pagesUnderstanding Learning Theories and Knowledge AcquisitionKarl Maloney Erfe100% (1)
- UNIT 1 Sociology - Lisening 2 Book Review of Blink by Malcolm GladwellDocument9 pagesUNIT 1 Sociology - Lisening 2 Book Review of Blink by Malcolm GladwellNgọc ÁnhNo ratings yet
- Coursebook 1Document84 pagesCoursebook 1houetofirmin2021No ratings yet
- Hydrocarbon LawDocument48 pagesHydrocarbon LawParavicoNo ratings yet
- Social Responsibility and Ethics in Marketing: Anupreet Kaur MokhaDocument7 pagesSocial Responsibility and Ethics in Marketing: Anupreet Kaur MokhaVlog With BongNo ratings yet
- 02 Activity 1 (4) (STRA)Document2 pages02 Activity 1 (4) (STRA)Kathy RamosNo ratings yet
- Sustainable Marketing and Consumers Preferences in Tourism 2167Document5 pagesSustainable Marketing and Consumers Preferences in Tourism 2167DanielNo ratings yet
- Ten Lessons (Not?) Learnt: Asset AllocationDocument30 pagesTen Lessons (Not?) Learnt: Asset AllocationkollingmNo ratings yet
- Summer 2011 Redwood Coast Land Conservancy NewsletterDocument6 pagesSummer 2011 Redwood Coast Land Conservancy NewsletterRedwood Coast Land ConservancyNo ratings yet
- Virtuoso 2011Document424 pagesVirtuoso 2011rraaccNo ratings yet
- 12 Smart Micro-Habits To Increase Your Daily Productivity by Jari Roomer Better Advice Oct, 2021 MediumDocument9 pages12 Smart Micro-Habits To Increase Your Daily Productivity by Jari Roomer Better Advice Oct, 2021 MediumRaja KhanNo ratings yet
- 2nd YearDocument5 pages2nd YearAnbalagan GNo ratings yet