You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Ford Everes PDFDocument584 pagesFord Everes PDFTiến Hồ100% (6)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- AASHTO GeoTechnical Design of PileDocument5 pagesAASHTO GeoTechnical Design of PiletrannguyenvietNo ratings yet
- Power Electronics - B. R. Gupta and v. SinghalDocument114 pagesPower Electronics - B. R. Gupta and v. SinghalHarish Kumar M50% (2)
- PumpDocument34 pagesPumpsoha89100% (1)
- Meritor Axle MT 40 143MA NDocument55 pagesMeritor Axle MT 40 143MA Nford62bNo ratings yet
- Architectural Drawing and Design PHS Syllabus 0910Document4 pagesArchitectural Drawing and Design PHS Syllabus 0910nourhanNo ratings yet
- SEMIKRON Product Catalogue 2014 2015Document167 pagesSEMIKRON Product Catalogue 2014 2015cesar oliveira0% (1)
- Three Mile Island AccidentDocument18 pagesThree Mile Island Accidentsoha89No ratings yet
- PumpsDocument32 pagesPumpssoha89100% (1)
- Fusion ScribdDocument10 pagesFusion ScribdSoha MakhyounNo ratings yet
- Gama Dimat Catalog Be17Document16 pagesGama Dimat Catalog Be17ELMIR ADILNo ratings yet
- Paradox Pir 476 Dg55 Dg55c Dg65 Dg65c Dg75 Dg75c 476 476pet Atm EtlDocument1 pageParadox Pir 476 Dg55 Dg55c Dg65 Dg65c Dg75 Dg75c 476 476pet Atm EtlTech StarNo ratings yet
- Operation Manual - A Table of ContentsDocument506 pagesOperation Manual - A Table of ContentsErvin PregNo ratings yet
- Física Práctica 1 MRUDocument5 pagesFísica Práctica 1 MRUPolet BarrionuevoNo ratings yet
- Benq mp510 Level1Document212 pagesBenq mp510 Level1Juan Duarte Lopez100% (1)
- Earthquake in TaguigDocument4 pagesEarthquake in TaguigDianca Zyra Rodil-CabanelaNo ratings yet
- West Beverly Homes-BoqDocument6 pagesWest Beverly Homes-BoqERICNo ratings yet
- Extra - Exercises Unistall InformixDocument14 pagesExtra - Exercises Unistall InformixМихаи БонцалоNo ratings yet
- SuperOrca ManualDocument22 pagesSuperOrca Manualarm usaNo ratings yet
- SW11Document6 pagesSW11Adam GordonNo ratings yet
- 80312A-ENUS Error LogDocument10 pages80312A-ENUS Error LogSafdar HussainNo ratings yet
- Ms2N Synchronous Servomotors: Project Planning ManualDocument408 pagesMs2N Synchronous Servomotors: Project Planning ManualGuido PerezNo ratings yet
- Assimilable Organic Carbon Formation During Ultraviolet - Hydrogen Peroxide Advanced Oxidation Treatment of Surface WaterDocument207 pagesAssimilable Organic Carbon Formation During Ultraviolet - Hydrogen Peroxide Advanced Oxidation Treatment of Surface WaterMonicaRossetimNo ratings yet
- Iei Pe MC PDFDocument3 pagesIei Pe MC PDFKulbir ThakurNo ratings yet
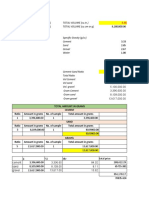
- Computation For Concrete Mix 120221Document3 pagesComputation For Concrete Mix 120221MASGRO BUILDERSNo ratings yet
- Hyundai Heavy Industries - Gas Insulated SwitchgearDocument25 pagesHyundai Heavy Industries - Gas Insulated SwitchgearbadbenzationNo ratings yet
- CS193a Android ProgrammingDocument4 pagesCS193a Android Programmingrosy01710No ratings yet
- 7 Basic Control ActionsDocument27 pages7 Basic Control ActionsAhmad ElsheemyNo ratings yet
- Operating Systems: Credits: 4 Credits Course Coordinator: V.V.SubrahmanyamDocument4 pagesOperating Systems: Credits: 4 Credits Course Coordinator: V.V.SubrahmanyamHarendra KumarNo ratings yet
- Valtra Tractor All Model Diagnostics and Programming ManualDocument22 pagesValtra Tractor All Model Diagnostics and Programming Manualpicax1879100% (17)
- ReactionsDocument30 pagesReactionskaloibestNo ratings yet
- Bicycle and Motorcycle DynamicsDocument36 pagesBicycle and Motorcycle DynamicsChanakya ChNo ratings yet
- CM P1CM EP1 Operation ManualDocument24 pagesCM P1CM EP1 Operation Manualnguyen vuNo ratings yet
- Design of Earth-Quake Resistant Multi Storied RCC Building On A Sloping GroundDocument24 pagesDesign of Earth-Quake Resistant Multi Storied RCC Building On A Sloping GroundKakula SasidharNo ratings yet