You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Foods Ot Avoid For Improved ADHD SymtomsDocument13 pagesFoods Ot Avoid For Improved ADHD Symtomsmanjunatha reddy100% (4)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Serological Techniques. Antigen-Antibody ReactionsDocument53 pagesSerological Techniques. Antigen-Antibody ReactionsHairul AnuarNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Clinical Applications of Nursing Diagnosis - Adult, Child, Women's, Psychiatric, Gerontic, and Home Health ConsDocument897 pagesClinical Applications of Nursing Diagnosis - Adult, Child, Women's, Psychiatric, Gerontic, and Home Health Consputri100% (3)
- Culture Bound SyndromesDocument14 pagesCulture Bound SyndromesLinda MathewNo ratings yet
- SUTGTielas LJ3231 HDocument38 pagesSUTGTielas LJ3231 HAndreea ChiriloiuNo ratings yet
- MDR in DetailsDocument370 pagesMDR in Detailssachin100% (2)
- RAdiology of HIVAIDSDocument928 pagesRAdiology of HIVAIDSbalNo ratings yet
- I. Single Population (Z Test & T Test)Document11 pagesI. Single Population (Z Test & T Test)Genette Sy Solis100% (1)
- Parad PurificationDocument9 pagesParad PurificationrajeshNo ratings yet
- NCP Ischemic StrokeDocument3 pagesNCP Ischemic StrokeEyySiEffVee100% (1)
- The Importance of Safety When Using AromatherapyDocument7 pagesThe Importance of Safety When Using AromatherapynanisoulaNo ratings yet
- Person Centered TherapyDocument16 pagesPerson Centered TherapyAldrinBalitaNo ratings yet
- Laboratory Diagnosis of InfectionDocument4 pagesLaboratory Diagnosis of InfectionHairul Anuar100% (1)
- Arixtra Drug StudyDocument2 pagesArixtra Drug StudyEdelweiss Marie Cayetano100% (1)
- Emotional and Behaviour DisorderDocument21 pagesEmotional and Behaviour DisorderBoingotlo Gosekwang100% (1)
- Terminal Illness and DeathDocument37 pagesTerminal Illness and DeathJAYSON KING100% (2)
- All WeeksDocument2 pagesAll WeeksQairul AzmanNo ratings yet
- Ticket Air Asia 13 Nov Ke Bangalore DuluDocument6 pagesTicket Air Asia 13 Nov Ke Bangalore DuluHairul AnuarNo ratings yet
- Cardiac Cycle: Presenter: DR Hairul Anuar Bin MahatDocument23 pagesCardiac Cycle: Presenter: DR Hairul Anuar Bin MahatHairul AnuarNo ratings yet
- Ranking Top 50Document5 pagesRanking Top 50Hairul AnuarNo ratings yet
- Module 8, 9Document1 pageModule 8, 9Hairul AnuarNo ratings yet
- Week 8Document4 pagesWeek 8Hairul AnuarNo ratings yet
- Module 8, 9Document1 pageModule 8, 9Hairul AnuarNo ratings yet
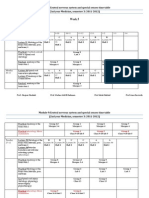
- Week 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Document10 pagesWeek 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Qairul AzmanNo ratings yet
- Microbiology: - Gram Positive BacilliDocument6 pagesMicrobiology: - Gram Positive BacilliHairul AnuarNo ratings yet
- CorrectionDocument2 pagesCorrectionHairul AnuarNo ratings yet
- All Weeks (Latest)Document10 pagesAll Weeks (Latest)Hairul AnuarNo ratings yet
- All Weeks (Latest)Document17 pagesAll Weeks (Latest)Hairul AnuarNo ratings yet
- EarDocument26 pagesEarHairul AnuarNo ratings yet
- Week 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Document17 pagesWeek 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Hairul AnuarNo ratings yet
- Week 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Document17 pagesWeek 5: Module 9:central Nervous System and Special Senses Time Table (2nd Year Medicine, Semester 3: 2011-2012)Hairul AnuarNo ratings yet
- Soalan 1st WeeksDocument14 pagesSoalan 1st WeeksQairul AzmanNo ratings yet
- Eye CataractDocument1 pageEye CataractHairul AnuarNo ratings yet
- 5-Lab Diagnosis of Fungal InfectionDocument12 pages5-Lab Diagnosis of Fungal InfectionHairul AnuarNo ratings yet
- Neurotransmitters 2Document35 pagesNeurotransmitters 2Hairul Anuar100% (2)
- 5-Lab Diagnosis of Fungal InfectionDocument12 pages5-Lab Diagnosis of Fungal InfectionHairul AnuarNo ratings yet
- 1 HelminthsDocument2 pages1 HelminthsHairul AnuarNo ratings yet
- Anatomy of The Head and Neck and EmbryologyDocument43 pagesAnatomy of The Head and Neck and EmbryologyHairul Anuar100% (1)
- 4-Disease Transmitting InsectaDocument10 pages4-Disease Transmitting InsectaHairul AnuarNo ratings yet
- Case ILA Final QuestionsDocument24 pagesCase ILA Final QuestionsHairul AnuarNo ratings yet
- Case ILA Final AnswersDocument45 pagesCase ILA Final AnswersHairul AnuarNo ratings yet
- 3-Crustacea and ArachnidaDocument3 pages3-Crustacea and ArachnidaHairul AnuarNo ratings yet
- 5-Major His To Compatibility Complex (MHC)Document12 pages5-Major His To Compatibility Complex (MHC)lianazulakNo ratings yet
- 4 Ab, Complement 3Document39 pages4 Ab, Complement 3lianazulakNo ratings yet
- Medical Equipment ListDocument10 pagesMedical Equipment Listamanuel waleluNo ratings yet
- Surgical Hand PreparationDocument28 pagesSurgical Hand PreparationyafetNo ratings yet
- Dissertation - 0207 (1) FinalDocument34 pagesDissertation - 0207 (1) FinalVP OFFICENo ratings yet
- Solomon Ankle Injury PDFDocument9 pagesSolomon Ankle Injury PDFHikmah Wahid AkbarNo ratings yet
- Direct Cuspal Coverage Posterior Resin Composite RestorationsDocument8 pagesDirect Cuspal Coverage Posterior Resin Composite Restorationsdentace1No ratings yet
- Root Canals: What To Expect During A ROOT CANALDocument3 pagesRoot Canals: What To Expect During A ROOT CANALKuntum Khaira UmmahNo ratings yet
- IDRAC - 359565 - 06-Feb-2023 - Summary of Community Decisions 2023 - C 37 - 01 - On Marketing Authorisations inDocument17 pagesIDRAC - 359565 - 06-Feb-2023 - Summary of Community Decisions 2023 - C 37 - 01 - On Marketing Authorisations inMahadeva BogegowdaNo ratings yet
- MinitrephDocument8 pagesMinitrephdisk_la_poduNo ratings yet
- Reduced Fare Program For People With DisabilitiesDocument4 pagesReduced Fare Program For People With DisabilitiesN SNo ratings yet
- Cape Verdean NewsletterDocument14 pagesCape Verdean Newsletterapi-397035932No ratings yet
- Final Nursing Skills Check-OffDocument17 pagesFinal Nursing Skills Check-OffWMG 10/10100% (1)
- AndermannDocument4 pagesAndermannButchay LumbabNo ratings yet
- Comparison of Joint Perception Between Posterior-Stabilized and Ultracongruent Total Knee Arthroplasty in The Same PatientDocument9 pagesComparison of Joint Perception Between Posterior-Stabilized and Ultracongruent Total Knee Arthroplasty in The Same PatientNuno PaisNo ratings yet
- Eng PDFDocument220 pagesEng PDFyunNo ratings yet
- Aplastic AnemiaDocument19 pagesAplastic AnemiaShara SampangNo ratings yet
- Normal H&P Write UpDocument4 pagesNormal H&P Write Upsonnynguyen208682No ratings yet