You might also like
- Kabiven: (Amino Acids, Electrolytes, Dextrose and Lipid Injectable Emulsion), For Intravenous UseDocument24 pagesKabiven: (Amino Acids, Electrolytes, Dextrose and Lipid Injectable Emulsion), For Intravenous UseDivine Mercy De JulianNo ratings yet
- Acute Inflammatory Demyelinating PolyneuropathyDocument55 pagesAcute Inflammatory Demyelinating PolyneuropathyImmanuel100% (1)
- Drug StudyDocument3 pagesDrug StudyKwin SaludaresNo ratings yet
- Osteomalacia Care Plan/OthersDocument11 pagesOsteomalacia Care Plan/OthersJill Jackson, RNNo ratings yet
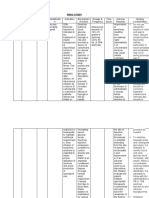
- Name of Drug General Action Specific Action Indications Contraindications Adverse Reaction Nursing ResponsibilitiesDocument1 pageName of Drug General Action Specific Action Indications Contraindications Adverse Reaction Nursing ResponsibilitiesNicole SooNo ratings yet
- What Is Stroke?: BY: Luis Alberto Sanchez Hernandez Physical TherapistDocument12 pagesWhat Is Stroke?: BY: Luis Alberto Sanchez Hernandez Physical TherapistLidiaAMonroyRNo ratings yet
- Case 1Document9 pagesCase 1Joselyn M. LachicaNo ratings yet
- Mesoridazine Drug StudyDocument5 pagesMesoridazine Drug Studyshadow gonzalezNo ratings yet
- Amitriptyline PDFDocument3 pagesAmitriptyline PDFscribdseewalNo ratings yet
- CCMH Drug StudyDocument5 pagesCCMH Drug StudyJoy JarinNo ratings yet
- Fluanxol Depot: Name of MedicineDocument11 pagesFluanxol Depot: Name of MedicineIvo_NichtNo ratings yet
- DioxelDocument1 pageDioxelJosselle Sempio CalientaNo ratings yet
- Understanding Myasthenia GravisDocument16 pagesUnderstanding Myasthenia Graviszarka wahid buxNo ratings yet
- IV Abra DineDocument1 pageIV Abra DineChris Ian Vincent OfongNo ratings yet
- Pharmacotherapy of AsthmaDocument53 pagesPharmacotherapy of AsthmaStella Aprilia NurNo ratings yet
- Apixaban 5 PDFDocument2 pagesApixaban 5 PDFWanie Al-basriNo ratings yet
- StreptokinaseDocument18 pagesStreptokinasedickyNo ratings yet
- Prescribed Fluanxol Depot dosage and administrationDocument4 pagesPrescribed Fluanxol Depot dosage and administrationHavier EsparagueraNo ratings yet
- Anatomy and PhysiologyDocument6 pagesAnatomy and PhysiologyJessica MakalintalNo ratings yet
- Drug StudyDocument8 pagesDrug StudyRizzi DeveraNo ratings yet
- NCP CvaDocument7 pagesNCP CvaEmerson SilverioNo ratings yet
- Cancer ChemotherapyDocument28 pagesCancer ChemotherapyFidelis LovelyNo ratings yet
- ColistinDocument2 pagesColistinGwyn RosalesNo ratings yet
- Diclofenac Sodium & Omeprazole Drug StudyDocument3 pagesDiclofenac Sodium & Omeprazole Drug StudyMelah MunchlaxNo ratings yet
- Sodium Valproate Uses, DosageDocument2 pagesSodium Valproate Uses, DosageKhairul KhairulNo ratings yet
- A Drug Study On: EpinephrineDocument16 pagesA Drug Study On: EpinephrineJay Jay JayyiNo ratings yet
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyNo ratings yet
- HaemaccelinfDocument9 pagesHaemaccelinfSisca YulistianaNo ratings yet
- OlanzapineDocument4 pagesOlanzapineJaica Jane BunadoNo ratings yet
- Stevens-Johnson Syndrome CASEDocument38 pagesStevens-Johnson Syndrome CASEChristy Rose AgrisNo ratings yet
- Panhypopituitarism: Causes, Signs, and TreatmentDocument22 pagesPanhypopituitarism: Causes, Signs, and TreatmentRocel Devilles100% (1)
- Drug StudyDocument3 pagesDrug StudyGail SantosNo ratings yet
- Urinalysis Procedure & ResultsDocument6 pagesUrinalysis Procedure & ResultsbobtagubaNo ratings yet
- DS BiperidenDocument3 pagesDS BiperidenbillyktoubattsNo ratings yet
- DRUGS Study OrigDocument17 pagesDRUGS Study OrigKiersten Karen Policarpio Verina100% (1)
- Lasilactone PI 201801Document9 pagesLasilactone PI 201801Shivam GuptaNo ratings yet
- Drug Study Form TJDocument4 pagesDrug Study Form TJJasmin Santiago CarrilloNo ratings yet
- MorphineDocument3 pagesMorphineAizat KamalNo ratings yet
- Hypovolemic Shock Concept MapDocument1 pageHypovolemic Shock Concept MapJM AsentistaNo ratings yet
- Esophageal DiverticulaDocument13 pagesEsophageal DiverticulaShekaira B. SimsimNo ratings yet
- Organophosphrous PoisoningDocument53 pagesOrganophosphrous Poisoningpriyashu78100% (1)
- Mood Stabilizing Drugs-Daga, JaDocument19 pagesMood Stabilizing Drugs-Daga, JaJoel Andrew Java DagaNo ratings yet
- Versed MidazolamDocument1 pageVersed MidazolamJan FuniestasNo ratings yet
- SeroquelDocument2 pagesSeroqueldanaNo ratings yet
- Acute Renal Failure Nursing Care PlanDocument15 pagesAcute Renal Failure Nursing Care PlanRanusha AnushaNo ratings yet
- Drug StudyDocument8 pagesDrug StudyzenNo ratings yet
- Lithium drug monitoring and toxicityDocument13 pagesLithium drug monitoring and toxicityGhee EvangelistaNo ratings yet
- SildenafilDocument2 pagesSildenafilSheryl Ann PedinesNo ratings yet
- Reteplase (MIRel)Document23 pagesReteplase (MIRel)Jhoann JamanilaNo ratings yet
- Drug Profile - AmantadinDocument14 pagesDrug Profile - AmantadinAna TanNo ratings yet
- P 398Document1 pageP 398Arup Ratan PaulNo ratings yet
- Drug AnalysisDocument3 pagesDrug Analysiskristel_nicole18yahoNo ratings yet
- Nursing responsibilities for atropine and diazepam drug studiesDocument4 pagesNursing responsibilities for atropine and diazepam drug studiesMarie Kris Chua AbelleraNo ratings yet
- Risk For SuicideDocument3 pagesRisk For SuicidepamfiestaNo ratings yet
- Drug Study - Epidural AnesthesiaDocument5 pagesDrug Study - Epidural AnesthesiaMarie PotayreNo ratings yet
- Drug Study - LevothyroxineDocument1 pageDrug Study - LevothyroxineCarla Tongson MaravillaNo ratings yet
- Antihypertensive AgentsDocument33 pagesAntihypertensive AgentsJuwairia tariqNo ratings yet
- 9 - Psychoactive Drugs - Chan, Marcayda, UyDocument19 pages9 - Psychoactive Drugs - Chan, Marcayda, UyCarlos Chan IVNo ratings yet
- Antiepileptics PD 501Document27 pagesAntiepileptics PD 501SidraNo ratings yet
- Taming The Id and Strengthening The Ego - Martha Stark MDDocument208 pagesTaming The Id and Strengthening The Ego - Martha Stark MDSasu NicoletaNo ratings yet
- Daftar Pustaka: Farmakologi Terapi. Goodman & Gilman. Edisi 10. Jakarta. EGC. H. 433-464Document5 pagesDaftar Pustaka: Farmakologi Terapi. Goodman & Gilman. Edisi 10. Jakarta. EGC. H. 433-464Muhammad FadhlurrohmanNo ratings yet
- Behaviour Problems in Children and HomoeopathyDocument6 pagesBehaviour Problems in Children and HomoeopathyHomoeopathic Pulse100% (1)
- MKULTRA Briefing Book SummaryDocument396 pagesMKULTRA Briefing Book SummaryTsz Kwan LiaoNo ratings yet
- R115Patients PDFDocument14 pagesR115Patients PDFcarneoliaNo ratings yet
- AcetaminophenDocument2 pagesAcetaminophendrugcardref100% (1)
- Applying Client-Centred Guidelines to Pediatric OTDocument7 pagesApplying Client-Centred Guidelines to Pediatric OTRaphael AguiarNo ratings yet
- Management Guidelines For Anxiety Disorders in Children and AdolescentsDocument23 pagesManagement Guidelines For Anxiety Disorders in Children and AdolescentsHari HaranNo ratings yet
- Celery Seed PDFDocument2 pagesCelery Seed PDFElviiSuhainiiSr.No ratings yet
- Journal Bedah Thorax 2Document15 pagesJournal Bedah Thorax 2Novia LarasatiNo ratings yet
- 2018 DPRI Booklet As of February 2019Document34 pages2018 DPRI Booklet As of February 2019kkabness101 YULNo ratings yet
- InlayDocument33 pagesInlayJitender Reddy75% (4)
- JVPDocument5 pagesJVPYhr YhNo ratings yet
- Tabela Grifo LaboratoryDocument11 pagesTabela Grifo LaboratoryGRIFO DIVULGA100% (2)
- Managerial accounting report on Homestead family clinic case studyDocument19 pagesManagerial accounting report on Homestead family clinic case studyIbrahim AmmarNo ratings yet
- Causes & Consequences of Drug AbuseDocument8 pagesCauses & Consequences of Drug AbuseamanbioqNo ratings yet
- Graves DseDocument5 pagesGraves DseHester Marie SimpiaNo ratings yet
- Cognitive Behavioral Model of Clinical Perfectionism Shafran Cooper Fairburn 2002 En-UsDocument1 pageCognitive Behavioral Model of Clinical Perfectionism Shafran Cooper Fairburn 2002 En-UsPavlov PicassoNo ratings yet
- 2441-3300 Kneehab Phy Brochure 2r16Document2 pages2441-3300 Kneehab Phy Brochure 2r16MVP Marketing and DesignNo ratings yet
- DECS Form 178ORIGINALDocument1 pageDECS Form 178ORIGINALJhon FurioNo ratings yet
- Breast Cancer Differential DiagnosesDocument5 pagesBreast Cancer Differential DiagnosesRayhanun MardhatillahNo ratings yet
- Child Psychiatric DisordersDocument8 pagesChild Psychiatric DisordersGaurang ShirwadkarNo ratings yet
- Clostridium Difficile Infection Fidaxomicin Esnm1Document11 pagesClostridium Difficile Infection Fidaxomicin Esnm1Pet UrNo ratings yet
- Intricate Internal Anatomy of Teeth and Its Clinical Significance in Endodontics - A ReviewDocument10 pagesIntricate Internal Anatomy of Teeth and Its Clinical Significance in Endodontics - A ReviewManjeevNo ratings yet
- Dutch Osteoporosis Physiotherapy FlowchartDocument1 pageDutch Osteoporosis Physiotherapy FlowchartyohanNo ratings yet
- How To Grow Medicinal MarijuanaDocument9 pagesHow To Grow Medicinal MarijuanaRoy HarperNo ratings yet
- Magic of TouchDocument28 pagesMagic of TouchkurniawatiNo ratings yet
- Stress Management ResourcesDocument58 pagesStress Management ResourcesKomal JoshiNo ratings yet
- Books About GroupsDocument25 pagesBooks About GroupsgerawenceNo ratings yet
- Accidental Intravenous Infusion of Air: A Concise ReviewDocument5 pagesAccidental Intravenous Infusion of Air: A Concise ReviewSiswand BIn Mohd AliNo ratings yet