You might also like
- Cardiology MCQsDocument5 pagesCardiology MCQsTessa Neilson75% (4)
- Nephrology MCQ PDFDocument7 pagesNephrology MCQ PDFreenarachelgeorge100% (4)
- Nephrology MCQSDocument16 pagesNephrology MCQSThana AlAnsari100% (5)
- Neurology Multiple Choice Questions With Explanations: Volume IIIFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IIIRating: 4.5 out of 5 stars4.5/5 (6)
- برومترك كلي د.فهيمDocument136 pagesبرومترك كلي د.فهيمAshraf Ismail100% (2)
- Harrison MCQ NephrologyDocument7 pagesHarrison MCQ Nephrologydrtpk80% (15)
- Board Reveiw Electrolyte Acid Base MCQ and AnswerDocument15 pagesBoard Reveiw Electrolyte Acid Base MCQ and AnswerEma100% (8)
- Rheumatology Multiple Choice Questions with ExplanationsFrom EverandRheumatology Multiple Choice Questions with ExplanationsRating: 4.5 out of 5 stars4.5/5 (6)
- Hopkins Medicine Review NephrologyDocument35 pagesHopkins Medicine Review NephrologyMuhammad Bilal50% (2)
- Nephrology TestDocument22 pagesNephrology TestRishi KNair100% (1)
- برومترك أمراض الكلىDocument36 pagesبرومترك أمراض الكلىTariq Zayan100% (4)
- Board Review: Nephrology: Wednesday, August 19Document65 pagesBoard Review: Nephrology: Wednesday, August 19Lina Abuarqoub67% (3)
- SCFHS NEPHRO MCQs DR. RANA ZAHID HAFEEZDocument52 pagesSCFHS NEPHRO MCQs DR. RANA ZAHID HAFEEZranazahidhafeez100% (1)
- Medicine Multiple Choise QuestionsDocument61 pagesMedicine Multiple Choise QuestionsjuanmoraheNo ratings yet
- Nephrology TestDocument112 pagesNephrology TestRapid Medicine50% (2)
- Renal Disease McqsDocument20 pagesRenal Disease McqsShankar Deshmukh100% (1)
- Top 10 Nephro Slides in Board ExamsDocument223 pagesTop 10 Nephro Slides in Board ExamsMirza Shaharyar Baig100% (2)
- Chapter 44. Azotemia and Urinary Abnormalities: MCQ'S For Medical Professionals CardiologyDocument70 pagesChapter 44. Azotemia and Urinary Abnormalities: MCQ'S For Medical Professionals CardiologyBkash Shah100% (1)
- ACP Board Review Nephrology 20052ndDocument35 pagesACP Board Review Nephrology 20052nddoctormido2010100% (1)
- Nephrology - Internal Medicine, Dr. A. MowafyDocument64 pagesNephrology - Internal Medicine, Dr. A. MowafyMohammed Risq100% (1)
- MCQ On Cardiology IDocument84 pagesMCQ On Cardiology IHarsh Oak50% (2)
- Nephrology ExamsDocument30 pagesNephrology Examsdhianne_garcia2001100% (1)
- General Medicine MCQDocument11 pagesGeneral Medicine MCQsami1218100% (3)
- MRCP NephrologyDocument394 pagesMRCP Nephrologyxplaind100% (8)
- MCQs IN MEDICINEDocument150 pagesMCQs IN MEDICINERITESH SINGH100% (1)
- 4 Git Liver McqsDocument30 pages4 Git Liver Mcqsjayswalramesh71% (14)
- 2 Medicine MCQs NephrologyDocument3 pages2 Medicine MCQs NephrologyDiwakesh C BNo ratings yet
- General Medicine MCQDocument73 pagesGeneral Medicine MCQkhalida shaik begumNo ratings yet
- MCQSDocument6 pagesMCQSkhuzaima9100% (1)
- Cardiology (300) MRCP Part 1 2014Document927 pagesCardiology (300) MRCP Part 1 2014elite949150% (2)
- Renal Path Q'sDocument20 pagesRenal Path Q'skank_sNo ratings yet
- Best of Five Mcqs For The Gastroenterology Sce PDFDocument315 pagesBest of Five Mcqs For The Gastroenterology Sce PDFSabry Anees100% (8)
- MRCPIPart 2 Mock TestDocument87 pagesMRCPIPart 2 Mock TestMuhammadMujtabaHashir100% (4)
- Internal Medicine McqsDocument15 pagesInternal Medicine Mcqsunlimited world100% (2)
- Internal Medicine Board ReviewDocument64 pagesInternal Medicine Board Reviewgrahamabra50% (2)
- 86 MRCP Part 2 Sample QuestionsDocument86 pages86 MRCP Part 2 Sample QuestionsJa Gh50% (2)
- MCQ in MedicineDocument18 pagesMCQ in MedicineEslamAlmassri75% (4)
- Medscape NephrologyDocument33 pagesMedscape Nephrologybarackobama08100% (2)
- GIT MCQs DR - Ahmed MowafyDocument15 pagesGIT MCQs DR - Ahmed Mowafya7wfNo ratings yet
- MCQ GastroenterologyDocument7 pagesMCQ GastroenterologyAdamImanNo ratings yet
- Emergency MCQDocument22 pagesEmergency MCQمعتز حرارةNo ratings yet
- Davidson's McqsDocument145 pagesDavidson's McqsSekhons Akademy100% (3)
- MCQs 1Document10 pagesMCQs 1Mostafa MahmoudNo ratings yet
- Chronic Kidney DiseaseDocument39 pagesChronic Kidney DiseaseMohmmadRjab SederNo ratings yet
- Renal PacesDocument4 pagesRenal PacesRebecca Teng Siew YanNo ratings yet
- Acute Kidney InjuryDocument48 pagesAcute Kidney InjuryAnggioppleNo ratings yet
- Gangguan Ginjal Akut ("Acute Kidney Injury") : Prof. Dr. Dr. Adrian Umboh, Sp.A (K)Document22 pagesGangguan Ginjal Akut ("Acute Kidney Injury") : Prof. Dr. Dr. Adrian Umboh, Sp.A (K)Hans NatanaelNo ratings yet
- AcuteKidneyInjury 000Document48 pagesAcuteKidneyInjury 000Judith HallNo ratings yet
- Chronic Renal FailureDocument7 pagesChronic Renal FailureSurya Dewi PrimawatiNo ratings yet
- Complications of Liver CirrhosisDocument42 pagesComplications of Liver CirrhosisdevantyNo ratings yet
- AKI in ChildrenDocument43 pagesAKI in ChildrenYonas AwgichewNo ratings yet
- Step Up To Medicine Chapter 03Document868 pagesStep Up To Medicine Chapter 03yanks1120No ratings yet
- UCSF Hospitalist HandbookDocument58 pagesUCSF Hospitalist Handbookniharjhatn100% (1)
- OsceDocument90 pagesOsce106a- 106001956No ratings yet
- Dr. Vineet ChaturvediDocument69 pagesDr. Vineet ChaturvediVinay PatilNo ratings yet
- WHO - Health Researchers GuideDocument235 pagesWHO - Health Researchers Guidejonlim78No ratings yet
- EMQs For The MRCOG Part 2-The Essential GuideDocument152 pagesEMQs For The MRCOG Part 2-The Essential GuideJuanda Raynaldi100% (1)
- Diagnosis of Gastrointestinal Bleeding in AdultsDocument8 pagesDiagnosis of Gastrointestinal Bleeding in AdultsSaeed Al-YafeiNo ratings yet
- IDF Edisi 8 2017 PDFDocument150 pagesIDF Edisi 8 2017 PDFAnnisaNo ratings yet
- A Step by Step Guide To Writing A Scientific ManusDocument19 pagesA Step by Step Guide To Writing A Scientific ManusSaeed Al-YafeiNo ratings yet
- How To Write A Journal ArticleDocument50 pagesHow To Write A Journal ArticleSaeed Al-Yafei80% (5)
- Who DMG PDFDocument65 pagesWho DMG PDFShelly Silvia BintangNo ratings yet
- Endnote 7 TrainingDocument84 pagesEndnote 7 TrainingSaeed Al-Yafei100% (2)
- Preparatory Lecture: Confounding and BiasDocument144 pagesPreparatory Lecture: Confounding and BiasSaeed Al-YafeiNo ratings yet
- Searching The LiteratureDocument144 pagesSearching The LiteratureSaeed Al-YafeiNo ratings yet
- How To Write A Scientific Original ArticleDocument67 pagesHow To Write A Scientific Original ArticleSaeed Al-YafeiNo ratings yet
- Obs Gynae DopplerDocument40 pagesObs Gynae DopplerSaeed Al-YafeiNo ratings yet
- Health Research MethodologyDocument245 pagesHealth Research MethodologyApollo Institute of Hospital Administration100% (1)
- Cognitive PsychologyDocument22 pagesCognitive PsychologySaeed Al-Yafei100% (6)
- Searching The LiteratureDocument144 pagesSearching The LiteratureSaeed Al-YafeiNo ratings yet
- Ethics of Preparatory CourseDocument60 pagesEthics of Preparatory CourseSaeed Al-YafeiNo ratings yet
- AMEE Guide Supplements - Workplace-Based Assessment As An Educational Tool. Guide Supplement 31.1-Viewpoint1Document2 pagesAMEE Guide Supplements - Workplace-Based Assessment As An Educational Tool. Guide Supplement 31.1-Viewpoint1Saeed Al-YafeiNo ratings yet
- Internal Medicine DoctorateDocument6 pagesInternal Medicine DoctorateSaeed Al-YafeiNo ratings yet
- Screening TestDocument20 pagesScreening TestSaeed Al-YafeiNo ratings yet
- Interactive LecturingDocument6 pagesInteractive LecturingSaeed Al-Yafei100% (1)
- AACE 2013 DM Consensus Statement 1Document48 pagesAACE 2013 DM Consensus Statement 1As-sifa KharismaNo ratings yet
- Skelly S Mcqs in Tropical MedicineDocument29 pagesSkelly S Mcqs in Tropical MedicineSaeed Al-Yafei92% (13)
- Philosophy of Internal Medicine - Osler and HinohaDocument3 pagesPhilosophy of Internal Medicine - Osler and HinohaSri ViisnnuNo ratings yet
- Ecg - Basics For The Anesthesiologists: Dr.K.M.LakshmanarajanDocument145 pagesEcg - Basics For The Anesthesiologists: Dr.K.M.LakshmanarajanKM Lakshmana RajanNo ratings yet
- Rheumatic Heart DiseaseDocument3 pagesRheumatic Heart DiseaseSanthosh.S.UNo ratings yet
- BM 9303 - Diagnostic and Therapeutic Equipment IDocument1 pageBM 9303 - Diagnostic and Therapeutic Equipment IMythily VedhagiriNo ratings yet
- Atrial Fibrillation 1Document15 pagesAtrial Fibrillation 1api-595122187No ratings yet
- Final patho-HCVDDocument2 pagesFinal patho-HCVDAlvin RamirezNo ratings yet
- Electrocardiogram ExaminationDocument13 pagesElectrocardiogram ExaminationayunisallehNo ratings yet
- Unstable Angina PectorisDocument34 pagesUnstable Angina PectoriserinmowokaNo ratings yet
- PDF - Local Services List For Medical Facilities in Saudi ArabiaDocument9 pagesPDF - Local Services List For Medical Facilities in Saudi ArabiaVivek Kumar VermaNo ratings yet
- 2013 - Doctors and Medical Services Munich BavariaDocument44 pages2013 - Doctors and Medical Services Munich BavariaJoe MullerNo ratings yet
- BLS ExamDocument4 pagesBLS ExammanalgalmutairiNo ratings yet
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDocument2 pagesStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaNo ratings yet
- Attachment 6 Acute Kidney Injury Assessment Pathway Ref 2739Document2 pagesAttachment 6 Acute Kidney Injury Assessment Pathway Ref 2739Health Brook100% (1)
- Fan 2018Document4 pagesFan 2018Илија РадосављевићNo ratings yet
- Renal DiseaseDocument4 pagesRenal DiseaseApril Lady Faith P. PaundogNo ratings yet
- Nephrotic Vs Nephritic SyndromeDocument80 pagesNephrotic Vs Nephritic Syndromevan016_bunnyNo ratings yet
- Advanced Cardiac Life SupportDocument28 pagesAdvanced Cardiac Life SupportAbdulrahman AlsayyedNo ratings yet
- Unstable Angina: DR Abdul Mateen Ansari, MD Professor and HOD General Medicine, Cimsh, LucknowDocument27 pagesUnstable Angina: DR Abdul Mateen Ansari, MD Professor and HOD General Medicine, Cimsh, LucknowCyntia KhairaniNo ratings yet
- Atrial Fibrillation CASE STUDYDocument2 pagesAtrial Fibrillation CASE STUDYChristianneMikeNo ratings yet
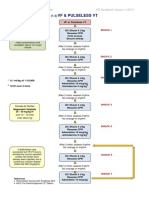
- VF & Pulseless VTDocument1 pageVF & Pulseless VTmadimadi11No ratings yet
- Full Programme 9Document18 pagesFull Programme 9Borneo CTVSNo ratings yet
- Cardiac Tamponade 2Document23 pagesCardiac Tamponade 2Jethro Floyd QuintoNo ratings yet
- ECG Practise Exam Answers - 2019Document10 pagesECG Practise Exam Answers - 2019Ronak SinaeiNo ratings yet
- ESC Guideline 2018Document84 pagesESC Guideline 2018Ganjar AdityoNo ratings yet
- Differences Aha and EuropeDocument3 pagesDifferences Aha and EuropeGilbertLiemNo ratings yet
- EACVI Multimodality Imaging of Native Valvular RegDocument62 pagesEACVI Multimodality Imaging of Native Valvular RegВенцислав МирчевNo ratings yet
- Oxy CadDocument21 pagesOxy CadrlinaoNo ratings yet
- Seram Anguillae (Eel Serum)Document2 pagesSeram Anguillae (Eel Serum)Shah FaisalNo ratings yet
- GREY BOOK August 2017 66thDocument146 pagesGREY BOOK August 2017 66thxedoyis969No ratings yet
- ECG (Cardiology Clinic 2006)Document127 pagesECG (Cardiology Clinic 2006)VuqarNo ratings yet