You might also like
- Drugs PharmacologyDocument75 pagesDrugs Pharmacologyapi-25987870100% (16)
- Krav Maga Pressure Points - Military Hand To Hand Combat GuideDocument27 pagesKrav Maga Pressure Points - Military Hand To Hand Combat Guidebrogan98% (135)
- Pharmacology Complete Drug TableDocument6 pagesPharmacology Complete Drug Tableninja-2001100% (4)
- Comprehensive Pharmacology SummaryDocument25 pagesComprehensive Pharmacology Summarysubash p100% (1)
- Pharmacology Illustrated Notes: Calcium Channel Blockers and DigoxinDocument148 pagesPharmacology Illustrated Notes: Calcium Channel Blockers and DigoxinShikha Khemani88% (8)
- Basic Principles of PharmacologyDocument47 pagesBasic Principles of Pharmacologysapiah raman100% (2)
- Pharm Drug ListDocument17 pagesPharm Drug Listanon_523534678No ratings yet
- 783 Q - 650 Answered 07.04.2019Document96 pages783 Q - 650 Answered 07.04.2019Syed Ibrahim100% (1)
- Drug of Choice and First Line of TreatmentDocument2 pagesDrug of Choice and First Line of Treatmentprinz1mendezNo ratings yet
- Pharma Katzung TablesDocument16 pagesPharma Katzung TablesPrincess Arabia-ObedozaNo ratings yet
- Super Fast Mental Math - Vedic Math HistoryDocument51 pagesSuper Fast Mental Math - Vedic Math Historyvedicmath98% (41)
- Cave Rescue ActivityDocument6 pagesCave Rescue Activityshweta bambuwalaNo ratings yet
- Pharmacology NotesDocument48 pagesPharmacology NotesBheru Lal100% (1)
- Drug Receptor Types: Cut Here Cut HereDocument60 pagesDrug Receptor Types: Cut Here Cut Heredlneisha61100% (13)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- PharmacologyDocument13 pagesPharmacologyMa Carmela GuevarraNo ratings yet
- Martial Arts - Bruce Lee's Speed TrainingDocument4 pagesMartial Arts - Bruce Lee's Speed Trainingbrogan97% (33)
- SympathomimeticsDocument25 pagesSympathomimeticsMirza Shaharyar BaigNo ratings yet
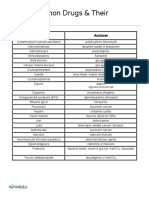
- Common Drugs and Their AntidotesDocument1 pageCommon Drugs and Their AntidoteskiranbhandarkarNo ratings yet
- Pharmacology Charts PDFDocument88 pagesPharmacology Charts PDFMohamad Samir90% (10)
- Drug Classification TableDocument6 pagesDrug Classification TableBouncesNo ratings yet
- Pharmacy MnenomicsDocument12 pagesPharmacy MnenomicsNaresh BabuNo ratings yet
- Pharm NotesDocument198 pagesPharm NotesNancy Danielz80% (5)
- Martial Arts - Bruce Lee's Training SecretsDocument3 pagesMartial Arts - Bruce Lee's Training Secretsbrogan91% (34)
- Respiratory and Cardiovascular DrugsDocument21 pagesRespiratory and Cardiovascular DrugsCandace Flowers100% (3)
- Pharmacology MnemonicsDocument19 pagesPharmacology MnemonicsAl-nazer Azer Al100% (5)
- Parasympathetic Pharmacology Drugs Muscarine and Nicotinic RecpetorsDocument56 pagesParasympathetic Pharmacology Drugs Muscarine and Nicotinic RecpetorsMatthewNo ratings yet
- MantrasDocument24 pagesMantrasg_gaurishankar@rediffmail.com100% (4)
- AntibioticsDocument2 pagesAntibioticsPGI Custodio, Ed KristianNo ratings yet
- SJDWHDJSDJSDDocument358 pagesSJDWHDJSDJSDwide mind hackerNo ratings yet
- Pharmacology OverviewDocument95 pagesPharmacology OverviewMiguel CuevasNo ratings yet
- Tally 9.2 NotesDocument1,918 pagesTally 9.2 NotesRamesh75% (4)
- Pharmacology List of DrugsDocument66 pagesPharmacology List of DrugsSohail Adnan100% (2)
- Muscarine & Nicotinic: ReceptorDocument26 pagesMuscarine & Nicotinic: ReceptorCess Lagera Ybanez88% (16)
- Pharmacology KatzDocument13 pagesPharmacology KatzFahd Abdullah Al-refaiNo ratings yet
- Pharmacology of SulphonamidesDocument21 pagesPharmacology of SulphonamidesGANESH KUMAR JELLA100% (1)
- Cytogenectics Reading ListDocument2 pagesCytogenectics Reading ListHassan GillNo ratings yet
- Classification of Drugs PDFDocument15 pagesClassification of Drugs PDFmuhammad ihtisham ul hassanNo ratings yet
- Adrenergic & Cholinergic DrugsDocument1 pageAdrenergic & Cholinergic DrugsMina Minawy100% (1)
- Pharmacology Drug ClassificationDocument4 pagesPharmacology Drug ClassificationRPh Krishna Chandra Jagrit100% (4)
- Adrenergic ReceptorsDocument9 pagesAdrenergic Receptorsrababmohsin110100% (1)
- PharmacologyDocument318 pagesPharmacologyAamir Sirohi94% (16)
- Pharmacology ReviewDocument172 pagesPharmacology ReviewJan Patrick Arrieta100% (1)
- Pharma ChartsDocument33 pagesPharma ChartsNooreen Hussain100% (1)
- Oracle Time and Labor - Data SheetDocument5 pagesOracle Time and Labor - Data Sheetbilaltanoli@gmail.comNo ratings yet
- Clinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsDocument26 pagesClinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsNadia Ancharuz100% (1)
- Pharmacology Mnemonics (Part 01) by M IhtishamDocument32 pagesPharmacology Mnemonics (Part 01) by M Ihtishammuhammad ihtisham ul hassan100% (1)
- Drug ClassificationDocument20 pagesDrug Classificationlizzeygail15No ratings yet
- Pharmacology BriefDocument287 pagesPharmacology BriefHu Mihi100% (1)
- Vijay Solvex PROJECT "Retention Strategy"Document110 pagesVijay Solvex PROJECT "Retention Strategy"Jayesh SinghNo ratings yet
- Mnemonics For Antibiotics-2Document10 pagesMnemonics For Antibiotics-2totallyfakeusernameNo ratings yet
- Rules & Guidelines of Elliott WaveDocument12 pagesRules & Guidelines of Elliott WaveNd Reyes100% (2)
- Niper Model Paper 1Document40 pagesNiper Model Paper 1GANESH KUMAR JELLANo ratings yet
- Sympathomimetic Drugs PharmacologyDocument10 pagesSympathomimetic Drugs PharmacologyHaroon JavedNo ratings yet
- Mantras - English - KundaliniDocument7 pagesMantras - English - KundaliniRPh Krishna Chandra JagritNo ratings yet
- OtcDocument10 pagesOtcJames PerianayagamNo ratings yet
- Niper Model Paper 4Document44 pagesNiper Model Paper 4RPh Krishna Chandra JagritNo ratings yet
- Vancomycin Pharmacology Indications, Mechanism, and Side Effects! PDFDocument1 pageVancomycin Pharmacology Indications, Mechanism, and Side Effects! PDFFrancis PasayNo ratings yet
- Antibiotic Summary - DraftDocument10 pagesAntibiotic Summary - DraftStrept Pneumonia100% (1)
- Antibiotics: Means Against LifeDocument13 pagesAntibiotics: Means Against Lifeshankul kumar100% (1)
- Pharmacology MCQsDocument12 pagesPharmacology MCQsSidharta ChatterjeeNo ratings yet
- Warfarin Sodium: INR Levels 4.0 or Less Ok To Carry Out Procedure Test Atleast 72 Hrs Prior To ProcedureDocument6 pagesWarfarin Sodium: INR Levels 4.0 or Less Ok To Carry Out Procedure Test Atleast 72 Hrs Prior To ProcedureVimi GeorgeNo ratings yet
- Drug interaction checkerDocument1 pageDrug interaction checkermadison61404100% (3)
- Sedative-Hypnotic and Antipsychotic Drugs GuideDocument17 pagesSedative-Hypnotic and Antipsychotic Drugs GuideBijay Kumar MahatoNo ratings yet
- SAR of Macrolides, Penicillins, and Other AntibioticsDocument36 pagesSAR of Macrolides, Penicillins, and Other AntibioticsBen Paolo Cecilia RabaraNo ratings yet
- Introduction To Cns PharmacologyDocument66 pagesIntroduction To Cns PharmacologyYazan Emad Salem100% (1)
- ANS Drug ClassificationDocument11 pagesANS Drug ClassificationUrugonda Venumadhav100% (1)
- Sympathomimetic Drug - WikipediaDocument5 pagesSympathomimetic Drug - Wikipediamohammedalradai629No ratings yet
- Chapter 17 Adrenergic AgonistsDocument13 pagesChapter 17 Adrenergic AgonistsKhalil MominNo ratings yet
- L19 - Adrenergic IVDocument7 pagesL19 - Adrenergic IVyasaira707No ratings yet
- Systemic Effects of Histamine and SerotoninDocument5 pagesSystemic Effects of Histamine and SerotoninibrahimNo ratings yet
- Sympathomimetics (Catecholamines & Non Catecholamines)Document99 pagesSympathomimetics (Catecholamines & Non Catecholamines)Raheel JavaidNo ratings yet
- L17 - Adrenergics IIDocument6 pagesL17 - Adrenergics IIyasaira707No ratings yet
- Chemical Interactions and Effects on the Nervous SystemDocument6 pagesChemical Interactions and Effects on the Nervous SystemCarlo Domingo LadieroNo ratings yet
- 1 SymphatomimeticsDocument10 pages1 SymphatomimeticsJericho De GuzmanNo ratings yet
- PDFDocument33 pagesPDFIvanes IgorNo ratings yet
- Meningioma TreatmentDocument9 pagesMeningioma TreatmentRPh Krishna Chandra JagritNo ratings yet
- About MeningiomaDocument5 pagesAbout MeningiomaRPh Krishna Chandra JagritNo ratings yet
- Matrimonial Resume CVDocument3 pagesMatrimonial Resume CVRPh Krishna Chandra Jagrit76% (37)
- Happy Birthday Nivisha... God Bless YouDocument1 pageHappy Birthday Nivisha... God Bless YouRPh Krishna Chandra JagritNo ratings yet
- RCJ CV-01 FinalDocument4 pagesRCJ CV-01 FinalRPh Krishna Chandra Jagrit100% (1)
- About This Tutorial: Version HistoryDocument328 pagesAbout This Tutorial: Version HistoryKate CorralesNo ratings yet
- Matrimonial Resume CVDocument3 pagesMatrimonial Resume CVRPh Krishna Chandra Jagrit76% (37)
- HTML-XHTML Tag SheDocument6 pagesHTML-XHTML Tag SheabcjohnNo ratings yet
- Matrimonial Resume CVDocument3 pagesMatrimonial Resume CVRPh Krishna Chandra Jagrit76% (37)
- Web DesigningDocument638 pagesWeb DesigningRPh Krishna Chandra JagritNo ratings yet
- Secret of The UniverseDocument26 pagesSecret of The UniverseRPh Krishna Chandra JagritNo ratings yet
- Niper Model Paper 5.Document47 pagesNiper Model Paper 5.GANESH KUMAR JELLANo ratings yet
- Tab CompleteDocument75 pagesTab CompleteGANESH KUMAR JELLANo ratings yet
- TocDocument72 pagesTocRPh Krishna Chandra JagritNo ratings yet
- Niper Model Paper 6.Document37 pagesNiper Model Paper 6.GANESH KUMAR JELLANo ratings yet
- Niper Model Paper 7.Document27 pagesNiper Model Paper 7.GANESH KUMAR JELLA100% (1)
- Niper Model Paper 7.Document27 pagesNiper Model Paper 7.GANESH KUMAR JELLA100% (1)
- Niper Model Paper 3.Document46 pagesNiper Model Paper 3.GANESH KUMAR JELLANo ratings yet
- Niper Model Paper 3.Document46 pagesNiper Model Paper 3.GANESH KUMAR JELLANo ratings yet
- Year 2 - Push and Pull FPDDocument18 pagesYear 2 - Push and Pull FPDRebecca LNo ratings yet
- Ultra Slimpak G448-0002: Bridge Input Field Configurable IsolatorDocument4 pagesUltra Slimpak G448-0002: Bridge Input Field Configurable IsolatorVladimirNo ratings yet
- Learn R For Applied StatisticsDocument457 pagesLearn R For Applied StatisticsyasortyNo ratings yet
- Yayasan Pendidikan Ramadanthy Milad Anniversary SpeechDocument6 pagesYayasan Pendidikan Ramadanthy Milad Anniversary SpeechDina Meyraniza SariNo ratings yet
- 1.an Overview On Membrane Strategies For Rare Earths Extraction and Separation - 2017Document36 pages1.an Overview On Membrane Strategies For Rare Earths Extraction and Separation - 2017Vasile AlexandraNo ratings yet
- Bimbo Marketing ResearchDocument27 pagesBimbo Marketing Researcheman.konsouhNo ratings yet
- Thesis PromptsDocument7 pagesThesis Promptsauroratuckernewyork100% (2)
- Vee 2003Document14 pagesVee 2003Syed faizan Ali zaidiNo ratings yet
- Curriculum Vitae: Name: Bhupal Shrestha Address: Kamalamai Municipality-12, Sindhuli, Nepal. Email: ObjectiveDocument1 pageCurriculum Vitae: Name: Bhupal Shrestha Address: Kamalamai Municipality-12, Sindhuli, Nepal. Email: Objectivebhupal shresthaNo ratings yet
- Ti 1000 0200 - enDocument2 pagesTi 1000 0200 - enJamil AhmedNo ratings yet
- Mapúa Welding Shop PracticeDocument7 pagesMapúa Welding Shop PracticeJay EmNo ratings yet
- MUM202001007 - 300 TR Price BOQ ChillerDocument4 pagesMUM202001007 - 300 TR Price BOQ ChillerB DASNo ratings yet
- Wilo Mather and Platt Pumps Pvt. LTD.: Technical DatasheetDocument2 pagesWilo Mather and Platt Pumps Pvt. LTD.: Technical DatasheetTrung Trần MinhNo ratings yet
- trac-nghiem-ngu-am-am-vi-hoc-tieng-anh-đã chuyển đổiDocument18 pagestrac-nghiem-ngu-am-am-vi-hoc-tieng-anh-đã chuyển đổiNguyễn ThiênNo ratings yet
- KOREADocument124 pagesKOREAchilla himmudNo ratings yet
- French Ox Cheek Stew with MushroomsDocument2 pagesFrench Ox Cheek Stew with MushroomsMihai LeancăNo ratings yet
- Case Study On Global Branding - DuluxDocument18 pagesCase Study On Global Branding - DuluxAakriti NegiNo ratings yet
- Fci FC CotsDocument25 pagesFci FC CotsMatthew DuNo ratings yet
- Working Capital Management (2015)Document62 pagesWorking Capital Management (2015)AJNo ratings yet
- Booklet English 2016Document17 pagesBooklet English 2016Noranita ZakariaNo ratings yet
- SPH3U Formula SheetDocument2 pagesSPH3U Formula SheetJSNo ratings yet
- RRLDocument4 pagesRRLTiltshifter ViNo ratings yet
- Nec TutorialDocument5 pagesNec TutorialbheemasenaNo ratings yet
- E TN SWD Csa A23 3 94 001 PDFDocument9 pagesE TN SWD Csa A23 3 94 001 PDFRazvan RobertNo ratings yet
- Modul English For Study SkillsDocument9 pagesModul English For Study SkillsRazan Nuhad Dzulfaqor razannuhad.2020No ratings yet