You might also like
- FalconryDocument25 pagesFalconryDragonMistressNo ratings yet
- Novice FalconryDocument87 pagesNovice Falconryx13x13100% (1)
- Hints on the Management of Hawks and Practical FalconryFrom EverandHints on the Management of Hawks and Practical FalconryNo ratings yet
- Eclectus Parrot. Eclectus Parrots as pets. Eclectus Parrot Keeping, Pros and Cons, Care, Housing, Diet and Health.From EverandEclectus Parrot. Eclectus Parrots as pets. Eclectus Parrot Keeping, Pros and Cons, Care, Housing, Diet and Health.No ratings yet
- Blue and Gold Macaws, The Complete Owner’s Guide on How to Care for Blue and Yellow Macaws, Facts on Habitat, Breeding, Lifespan, Behavior, Diet, Cages, Talking and Suitability as PetsFrom EverandBlue and Gold Macaws, The Complete Owner’s Guide on How to Care for Blue and Yellow Macaws, Facts on Habitat, Breeding, Lifespan, Behavior, Diet, Cages, Talking and Suitability as PetsRating: 5 out of 5 stars5/5 (1)
- The Minds and Manners of Wild Animals: A Book of Personal ObservationsFrom EverandThe Minds and Manners of Wild Animals: A Book of Personal ObservationsNo ratings yet
- Falconry Guide - Public Edition (SM)Document32 pagesFalconry Guide - Public Edition (SM)Agung Satriya Wibowo100% (2)
- Hawks at a Distance: Identification of Migrant RaptorsFrom EverandHawks at a Distance: Identification of Migrant RaptorsRating: 4.5 out of 5 stars4.5/5 (6)
- Wild Plants for Cage Birds - Weed and Seeds of the Field and Wayside Described - With Footnotes, etc., by G. E. WestonFrom EverandWild Plants for Cage Birds - Weed and Seeds of the Field and Wayside Described - With Footnotes, etc., by G. E. WestonNo ratings yet
- Falconry TermsDocument4 pagesFalconry Termsgonnaboy100% (1)
- Falconry: Perigrinus) Are Some of The More Commonly Used Birds of Prey. The Practice ofDocument19 pagesFalconry: Perigrinus) Are Some of The More Commonly Used Birds of Prey. The Practice ofLeonardo Miranda CollantesNo ratings yet
- Varanoid Lizards of the WorldFrom EverandVaranoid Lizards of the WorldErick PiankaRating: 5 out of 5 stars5/5 (2)
- California Hawking Club Test GuideDocument128 pagesCalifornia Hawking Club Test Guidegonnaboy100% (13)
- Raptor Nutrition enDocument39 pagesRaptor Nutrition enMark AbellaNo ratings yet
- Falcon ApprenticeDocument3 pagesFalcon ApprenticeState of UtahNo ratings yet
- Raptor ManualDocument75 pagesRaptor ManualCarlos Juan Martínez Pámanes100% (1)
- Practical Falconry PDFDocument106 pagesPractical Falconry PDFMichael Lennon de Moura100% (1)
- Falc GuideDocument28 pagesFalc GuideMark AbellaNo ratings yet
- Falconry Information ChecklistDocument5 pagesFalconry Information Checklisttoha putraNo ratings yet
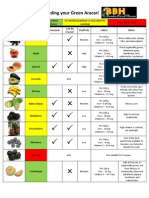
- Produce Guide For Feeding Your Green AracariDocument5 pagesProduce Guide For Feeding Your Green AracariaracariNo ratings yet
- Apprenticeship GuideDocument29 pagesApprenticeship GuideRotiseria La Flamme100% (2)
- Emergency Care of RaptorsDocument24 pagesEmergency Care of RaptorsjudithNo ratings yet
- Interpretation of The Reptile Blood ProfileDocument8 pagesInterpretation of The Reptile Blood ProfileAndre NgoNo ratings yet
- Urological Disorders of The Dog and CatDocument177 pagesUrological Disorders of The Dog and CatChiruc AmaliaNo ratings yet
- Avian Medicine PDFDocument1,384 pagesAvian Medicine PDFCamila Dergam100% (5)
- Self-Assessment Colour Review OF Avian MedicineDocument193 pagesSelf-Assessment Colour Review OF Avian MedicineXimenaPantiPrieto100% (1)
- EXOTİC-Raptor Medicine, Basic Principles and Noninfectious ConditionsDocument9 pagesEXOTİC-Raptor Medicine, Basic Principles and Noninfectious Conditionstaner_soysuren100% (1)
- Scarlet Macaw DietDocument8 pagesScarlet Macaw DietgabrielwerneckNo ratings yet
- Caring For Injured Reptiles2004Document40 pagesCaring For Injured Reptiles2004SujayJainNo ratings yet
- Haginbalds Arte of Medieval FaulconryDocument23 pagesHaginbalds Arte of Medieval FaulconryimmortalskyNo ratings yet
- Exotic Birds NutritionDocument21 pagesExotic Birds NutritiongabrielwerneckNo ratings yet
- JOSEPH 2006 Raptor Medicine - An Approach To Wild, Falconry, and Educational Birds of PreyDocument25 pagesJOSEPH 2006 Raptor Medicine - An Approach To Wild, Falconry, and Educational Birds of PreyigorvetNo ratings yet
- Falconry Sau Soimarit in UKDocument44 pagesFalconry Sau Soimarit in UKbenzzenhdNo ratings yet
- Veterinary Orthopedic Surgical Instuments CatalogDocument106 pagesVeterinary Orthopedic Surgical Instuments CatalogGerMedUsa.Com100% (1)
- Feather Destructive BehaviorDocument20 pagesFeather Destructive BehaviorAnh-MinhNo ratings yet
- Mammalian Diseases Found in Captivity FinalDocument45 pagesMammalian Diseases Found in Captivity Finalapi-250146149No ratings yet
- ParrotsDocument304 pagesParrotstobiasaxo5653No ratings yet
- Parrot Breeding and Keeping:: The Impact of Capture and CaptivityDocument66 pagesParrot Breeding and Keeping:: The Impact of Capture and CaptivityOjeda BorisNo ratings yet
- Pigeon Disease TreatmentsDocument1 pagePigeon Disease Treatmentsstevens75788No ratings yet
- Falconry - Celebrating A Living HeritageDocument11 pagesFalconry - Celebrating A Living HeritagebooksarabiaNo ratings yet
- 2003 Avian Care Manual PDFDocument132 pages2003 Avian Care Manual PDFRonald ChavezNo ratings yet
- Reptile Nutritional DiseasesDocument9 pagesReptile Nutritional DiseasesDiah PiastutiNo ratings yet
- Clinical Veterinary Advisor, 3rd Edition BabesiosisDocument5 pagesClinical Veterinary Advisor, 3rd Edition Babesiosisbio_trip160% (1)
- Nutritional Needs of Companion BirdsDocument33 pagesNutritional Needs of Companion BirdsHenrique Luís TavaresNo ratings yet
- Avian Hematology and Related DisordersDocument22 pagesAvian Hematology and Related DisordersIban Hernández100% (1)
- Anesthesia of Pet BirdsDocument12 pagesAnesthesia of Pet Birdstrung5848No ratings yet
- Practical Raptor Nutrition Neil Forbes PDFDocument9 pagesPractical Raptor Nutrition Neil Forbes PDFWisnu JuliastitoNo ratings yet
- Diagnostic Imaging of Exotic Pets Birds, Small Mammals, Reptiles - oDocument468 pagesDiagnostic Imaging of Exotic Pets Birds, Small Mammals, Reptiles - oAna Inés Erias67% (6)
- PW Book SampleDocument17 pagesPW Book SampleNina Sapphire100% (1)
- Case StudyDocument2 pagesCase StudyBunga Larangan73% (11)
- Attributes and DialogsDocument29 pagesAttributes and DialogsErdenegombo MunkhbaatarNo ratings yet
- IGCSE Chemistry Section 5 Lesson 3Document43 pagesIGCSE Chemistry Section 5 Lesson 3Bhawana SinghNo ratings yet
- To Introduce BgjgjgmyselfDocument2 pagesTo Introduce Bgjgjgmyselflikith333No ratings yet
- Pom Final On Rice MillDocument21 pagesPom Final On Rice MillKashif AliNo ratings yet
- Thin Film Deposition TechniquesDocument20 pagesThin Film Deposition TechniquesShayan Ahmad Khattak, BS Physics Student, UoPNo ratings yet
- Preventing and Mitigating COVID-19 at Work: Policy Brief 19 May 2021Document21 pagesPreventing and Mitigating COVID-19 at Work: Policy Brief 19 May 2021Desy Fitriani SarahNo ratings yet
- Forensic Science From The Crime Scene To The Crime Lab 2nd Edition Richard Saferstein Test BankDocument36 pagesForensic Science From The Crime Scene To The Crime Lab 2nd Edition Richard Saferstein Test Bankhilaryazariaqtoec4100% (25)
- 3ccc PDFDocument20 pages3ccc PDFKaka KunNo ratings yet
- Report Emerging TechnologiesDocument97 pagesReport Emerging Technologiesa10b11No ratings yet
- STAT100 Fall19 Test 2 ANSWERS Practice Problems PDFDocument23 pagesSTAT100 Fall19 Test 2 ANSWERS Practice Problems PDFabutiNo ratings yet
- 3 - Performance Measurement of Mining Equipments by Utilizing OEEDocument8 pages3 - Performance Measurement of Mining Equipments by Utilizing OEEGonzalo GarciaNo ratings yet
- AgentScope: A Flexible Yet Robust Multi-Agent PlatformDocument24 pagesAgentScope: A Flexible Yet Robust Multi-Agent PlatformRijalNo ratings yet
- Innovation Through Passion: Waterjet Cutting SystemsDocument7 pagesInnovation Through Passion: Waterjet Cutting SystemsRomly MechNo ratings yet
- Sentinel 2 Products Specification DocumentDocument510 pagesSentinel 2 Products Specification DocumentSherly BhengeNo ratings yet
- Astera Data Integration BootcampDocument4 pagesAstera Data Integration BootcampTalha MehtabNo ratings yet
- Level 3 Repair PBA Parts LayoutDocument32 pagesLevel 3 Repair PBA Parts LayoutabivecueNo ratings yet
- Evaluating Sources IB Style: Social 20ib Opvl NotesDocument7 pagesEvaluating Sources IB Style: Social 20ib Opvl NotesRobert ZhangNo ratings yet
- PRODUCTDocument82 pagesPRODUCTSrishti AggarwalNo ratings yet
- Wasserman Chest 1997Document13 pagesWasserman Chest 1997Filip BreskvarNo ratings yet
- Lecture Ready 01 With Keys and TapescriptsDocument157 pagesLecture Ready 01 With Keys and TapescriptsBảo Châu VươngNo ratings yet
- CR Vs MarubeniDocument15 pagesCR Vs MarubeniSudan TambiacNo ratings yet
- FranklinDocument4 pagesFranklinapi-291282463No ratings yet
- 2010 - Impact of Open Spaces On Health & WellbeingDocument24 pages2010 - Impact of Open Spaces On Health & WellbeingmonsNo ratings yet
- Phys101 CS Mid Sem 16 - 17Document1 pagePhys101 CS Mid Sem 16 - 17Nicole EchezonaNo ratings yet
- Marine Engineering 1921Document908 pagesMarine Engineering 1921Samuel Sneddon-Nelmes0% (1)
- Rounded Scoodie Bobwilson123 PDFDocument3 pagesRounded Scoodie Bobwilson123 PDFStefania MoldoveanuNo ratings yet
- Sri S T Kalairaj, Chairman: Income Tax TaxesDocument3 pagesSri S T Kalairaj, Chairman: Income Tax TaxesvikramkkNo ratings yet
- August 03 2017 Recalls Mls (Ascpi)Document6 pagesAugust 03 2017 Recalls Mls (Ascpi)Joanna Carel Lopez100% (3)
- Riddles For KidsDocument15 pagesRiddles For KidsAmin Reza100% (8)