You might also like
- Formulating An Agenda For The Women's Movement: A Review of NaripokkhoDocument7 pagesFormulating An Agenda For The Women's Movement: A Review of NaripokkhoHtaed TnawiNo ratings yet
- Hiv Aids Sex Work BangladeshDocument14 pagesHiv Aids Sex Work BangladeshHtaed TnawiNo ratings yet
- PracticalAnthropology MalinoswkiDocument17 pagesPracticalAnthropology MalinoswkiNacho TravadelaNo ratings yet
- WRITING Research ProposalDocument5 pagesWRITING Research ProposalHtaed TnawiNo ratings yet
- Nor PlantDocument20 pagesNor PlantHtaed TnawiNo ratings yet
- 2952557Document26 pages2952557Htaed TnawiNo ratings yet
- SullivanDocument7 pagesSullivanHtaed TnawiNo ratings yet
- 120 Chapter 5: Human Rights and Gender Equality: - 2010 Global ReportDocument24 pages120 Chapter 5: Human Rights and Gender Equality: - 2010 Global ReportHtaed TnawiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Term Paper On BF SkinnerDocument7 pagesTerm Paper On BF Skinnerc5rga5h2100% (1)
- Httpswww.ceec.Edu.twfilesfile Pool10j07580923432342090202 97指考英文試卷 PDFDocument8 pagesHttpswww.ceec.Edu.twfilesfile Pool10j07580923432342090202 97指考英文試卷 PDFAurora ZengNo ratings yet
- ZZXCDocument2 pagesZZXCKrisleen AbrenicaNo ratings yet
- G11SLM10.1 Oral Com Final For StudentDocument24 pagesG11SLM10.1 Oral Com Final For StudentCharijoy FriasNo ratings yet
- Edpb 506 Intergrated Unit Project RubricDocument1 pageEdpb 506 Intergrated Unit Project Rubricapi-487414247No ratings yet
- Apple Inc.: Managing Global Supply Chain: Case AnalysisDocument9 pagesApple Inc.: Managing Global Supply Chain: Case AnalysisPrateek GuptaNo ratings yet
- Navavarana ArticleDocument9 pagesNavavarana ArticleSingaperumal NarayanaNo ratings yet
- CA - Indonesia Digital Business Trend Final 2 Agust 2017Document38 pagesCA - Indonesia Digital Business Trend Final 2 Agust 2017silver8700No ratings yet
- Geraads 2016 Pleistocene Carnivora (Mammalia) From Tighennif (Ternifine), AlgeriaDocument45 pagesGeraads 2016 Pleistocene Carnivora (Mammalia) From Tighennif (Ternifine), AlgeriaGhaier KazmiNo ratings yet
- Ck-Nac FsDocument2 pagesCk-Nac Fsadamalay wardiwiraNo ratings yet
- Prof Ed 7 ICT Policies and Issues Implications To Teaching and LearningDocument11 pagesProf Ed 7 ICT Policies and Issues Implications To Teaching and Learnings.angelicamoradaNo ratings yet
- MT 1 Combined Top 200Document3 pagesMT 1 Combined Top 200ShohanNo ratings yet
- Strategic Planning and Program Budgeting in Romania RecentDocument6 pagesStrategic Planning and Program Budgeting in Romania RecentCarmina Ioana TomariuNo ratings yet
- English FinalDocument321 pagesEnglish FinalManuel Campos GuimeraNo ratings yet
- Reading and Writing Skills: Quarter 4 - Module 1Document16 pagesReading and Writing Skills: Quarter 4 - Module 1Ericka Marie AlmadoNo ratings yet
- LESSON 2 - Nguyễn Thu Hồng - 1917710050Document2 pagesLESSON 2 - Nguyễn Thu Hồng - 1917710050Thu Hồng NguyễnNo ratings yet
- Math 8 1 - 31Document29 pagesMath 8 1 - 31Emvie Loyd Pagunsan-ItableNo ratings yet
- Temperature Rise HV MotorDocument11 pagesTemperature Rise HV Motorashwani2101No ratings yet
- Unit 2 - Programming of 8085 MicroprocessorDocument32 pagesUnit 2 - Programming of 8085 MicroprocessorSathiyarajNo ratings yet
- English Course SyllabusDocument3 pagesEnglish Course Syllabusalea rainNo ratings yet
- Feminism in Lucia SartoriDocument41 pagesFeminism in Lucia SartoriRaraNo ratings yet
- Revision Summary - Rainbow's End by Jane Harrison PDFDocument47 pagesRevision Summary - Rainbow's End by Jane Harrison PDFchris100% (3)
- Best Safety Practices in The Philippine Construction PDFDocument16 pagesBest Safety Practices in The Philippine Construction PDFDione Klarisse GuevaraNo ratings yet
- The Role of Store LocationDocument6 pagesThe Role of Store LocationJessa La Rosa MarquezNo ratings yet
- Onkyo TX NR555 ManualDocument100 pagesOnkyo TX NR555 ManualSudhit SethiNo ratings yet
- NDA Template Non Disclosure Non Circumvent No Company NameDocument9 pagesNDA Template Non Disclosure Non Circumvent No Company NamepvorsterNo ratings yet
- Unitrain I Overview enDocument1 pageUnitrain I Overview enDragoi MihaiNo ratings yet
- AC & Crew Lists 881st 5-18-11Document43 pagesAC & Crew Lists 881st 5-18-11ywbh100% (2)
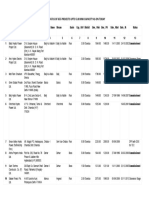
- List/Status of 655 Projects Upto 5.00 MW Capacity As On TodayDocument45 pagesList/Status of 655 Projects Upto 5.00 MW Capacity As On Todayganvaqqqzz21No ratings yet
- Surah Al A'araf (7:74) - People of ThamudDocument2 pagesSurah Al A'araf (7:74) - People of ThamudMuhammad Awais TahirNo ratings yet