You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Letter To Boingo RE - Free WifiDocument3 pagesLetter To Boingo RE - Free Wifiahawkins8223No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 2nd Circ SECDocument17 pages2nd Circ SECDanRivoliNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- United States Court of Appeals: For The First CircuitDocument35 pagesUnited States Court of Appeals: For The First CircuitDanRivoliNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- DOJ Healthcare Letter 040512Document3 pagesDOJ Healthcare Letter 040512pelofskyjNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Https Ecf Wied UscourtsDocument4 pagesHttps Ecf Wied UscourtsDanRivoliNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Judge Rejects Citigroup Settlement With SECDocument15 pagesJudge Rejects Citigroup Settlement With SECFindLawNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Beeson DKT 1-2 Docs From State CourtDocument52 pagesBeeson DKT 1-2 Docs From State CourtjohngaultNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Riverside Center StringerDocument22 pagesRiverside Center StringerDanRivoliNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Carry and Conceal Letter 10 19 11Document2 pagesCarry and Conceal Letter 10 19 11DanRivoliNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
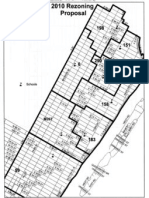
- Rezoning Map.Document1 pageRezoning Map.DanRivoliNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Respect The LaneDocument10 pagesRespect The LaneDanRivoliNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Seniors Bway Amst 71 SlidesDocument10 pagesSeniors Bway Amst 71 SlidesDanRivoliNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Debate FlierDocument1 pageDebate FlierDanRivoliNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Brewer Member ItemsDocument4 pagesBrewer Member ItemsDanRivoliNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- 2008 Drug Trend ReportDocument108 pages2008 Drug Trend Report阿龟100% (2)
- Nueces County Hospital District Christus SpohnDocument19 pagesNueces County Hospital District Christus SpohncallertimesNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- United States v. Franklin-El, 555 F.3d 1115, 10th Cir. (2009)Document25 pagesUnited States v. Franklin-El, 555 F.3d 1115, 10th Cir. (2009)Scribd Government DocsNo ratings yet
- Aldrete Discharge Scoring - Appropriate For Post Anesthesia Phase PDFDocument29 pagesAldrete Discharge Scoring - Appropriate For Post Anesthesia Phase PDFSurya BugisNo ratings yet
- NHS FPX 6008 Assessment 1 Identifying A Local Health Care Economic IssueDocument7 pagesNHS FPX 6008 Assessment 1 Identifying A Local Health Care Economic Issuezadem5266No ratings yet
- PSYCHIATRIC SOLUTIONS INC 10-K (Annual Reports) 2009-02-25Document89 pagesPSYCHIATRIC SOLUTIONS INC 10-K (Annual Reports) 2009-02-25http://secwatch.com100% (1)
- 2015 Uc Health FaaDocument4 pages2015 Uc Health Faaapi-263913260No ratings yet
- HCIA Study Guide 2023Document22 pagesHCIA Study Guide 2023consultasluisfloresdrNo ratings yet
- CVS Caremark Q MonthlyDocument2 pagesCVS Caremark Q MonthlyAngie Henderson MoncadaNo ratings yet
- Test Bank For Medical Surgical Nursing Concepts and Practice 1st Edition DewitDocument26 pagesTest Bank For Medical Surgical Nursing Concepts and Practice 1st Edition Dewitansauglyrk68l3100% (30)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 5 Quality Measures That Matter For Value-Based CareDocument8 pages5 Quality Measures That Matter For Value-Based CareTuan Nguyen DangNo ratings yet
- Nur 330 FinalDocument12 pagesNur 330 Finalapi-541785084No ratings yet
- Long Term LivingDocument168 pagesLong Term LivingJohann Victorious-Redd SmithNo ratings yet
- Joint Response by Texas HHSC, DFPS To CWOP Expert Panel RecommendationsDocument9 pagesJoint Response by Texas HHSC, DFPS To CWOP Expert Panel RecommendationsdmnpoliticsNo ratings yet
- Understanding Medicare/ Entendiendo MedicareDocument13 pagesUnderstanding Medicare/ Entendiendo MedicareEmily RamosNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- OASIS-E Guidance Manual - 5.16.22Document396 pagesOASIS-E Guidance Manual - 5.16.22mosaNo ratings yet
- Gonzales Cannon April 11 IssueDocument24 pagesGonzales Cannon April 11 IssueGonzales CannonNo ratings yet
- Durable Medical Equipment Reuse and Recycling: Uncovering Hidden Opportunities For Reducing Medical WasteDocument9 pagesDurable Medical Equipment Reuse and Recycling: Uncovering Hidden Opportunities For Reducing Medical WasteSebastián MeraNo ratings yet
- Eligibility Notice: Take Action To Enroll & Use Your Financial HelpDocument11 pagesEligibility Notice: Take Action To Enroll & Use Your Financial HelpJOENo ratings yet
- Texas Government Term Paper TopicsDocument8 pagesTexas Government Term Paper Topicsc5eyjfntNo ratings yet
- Culture Change in Elder Care (Excerpt)Document10 pagesCulture Change in Elder Care (Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.No ratings yet
- Dalrymple's State of The State AddressDocument10 pagesDalrymple's State of The State AddressRob PortNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sleep Deprivation PowerpointDocument24 pagesSleep Deprivation Powerpointapi-302310876100% (1)
- Medicaid Asset Protection LadyBirdDeedsinTexasDocument12 pagesMedicaid Asset Protection LadyBirdDeedsinTexasLISHA STONENo ratings yet
- CVS 10kDocument213 pagesCVS 10kSaitama UniverseNo ratings yet
- 7 Pillars of Effective Ethics and Compliance Program Soru 2Document2 pages7 Pillars of Effective Ethics and Compliance Program Soru 2sezo6No ratings yet
- DHA Exam SampleDocument5 pagesDHA Exam SampleMaddy Sweet50% (2)
- Non-Emergency Medical Transportation For Traditional Medicaid: Southeastrans Frequently Asked QuestionsDocument22 pagesNon-Emergency Medical Transportation For Traditional Medicaid: Southeastrans Frequently Asked QuestionsIndiana Family to FamilyNo ratings yet
- Understanding Dependency by David EllwoodDocument29 pagesUnderstanding Dependency by David EllwoodvwkyangNo ratings yet
- ABG GMC Policy 2016-17 - Management CadreDocument10 pagesABG GMC Policy 2016-17 - Management CadreAnonymous dGnj3bZNo ratings yet
- The Courage to Be Free: Florida's Blueprint for America's RevivalFrom EverandThe Courage to Be Free: Florida's Blueprint for America's RevivalNo ratings yet