DECLARATION
Declaration made this ______ day of ____________________, _____. I, Dorian Mayhew Rothschild, being of sound mind, willfully and voluntarily make known my desires that my dying shall not be artificially prolonged under the circumstances set forth below, hereby declare: A. LIFE-SUSTAINING PROCEDURES. If at any time I should have an incurable injury, disease, or illness certified to be a terminal condition or a permanently unconscious condition by two physicians who have personally examined me, one of whom shall be my attending physician, and the physicians have determined that my death will occur within a relatively short time, or that I will remain in a permanently unconscious condition, and where the application of life-sustaining procedures would serve only to artificially prolong the dying process, I direct that such procedures be withheld or withdrawn, and that I be permitted to die naturally with only the administration of medication or the performance of any medical procedure deemed necessary to provide me with comfort care. B. NUTRITION AND HYDRATION. If I have a condition stated above, it is my preference NOT TO RECEIVE artificially administered nutrition and hydration (food and fluids), except as deemed necessary to provide me with comfort care. If any provision in this document is held to be invalid, such invalidity shall not affect the other provisions which can be given effect without the invalid provision, and to this end the directions in this document are severable. In the absence of my ability to give directions regarding the use of such life-sustaining procedures, it is my intention that this Declaration shall be honored by my family physician(s) as the final expression of my legal right to refuse medical or surgical treatment and accept the consequences from such refusal.
I fully understand that action taken in accordance with this declaration might result in my death, and I am emotionally and mentally competent to make this declaration.
This is a RocketLawyer.com Legal Document
Date Signed: ____________________ ______, _____.
Signature: Name: Address:
________________________________________ Dorian Mayhew Rothschild 60 Arthur St. San Rafael Darton County Michigan 123-45-6789 February 23, 1965
SSN: Birthdate:
Dorian Mayhew Rothschild, the Declarant, has been personally known to me and appears to be of sound mind and under no duress, fraud, or undue influence. I am not (i) Dorian Mayhew Rothschild's spouse, parent, child, grandchild, sibling, (ii) entitled to any portion of the estate of Dorian Mayhew Rothschild according to the laws of Intestate Succession or under any will or codicil of Dorian Mayhew Rothschild, (iii) Dorian Mayhew Rothschild's physician or patient advocate, (iv) an employee of a home for the aged where Dorian Mayhew Rothschild resides, (v) an employee of a health facility that is treating Dorian Mayhew Rothschild, or (vi) an employee of a life or health insurance provider for the patient. I am at least 18 years of age.
Witness Signature: Name: Address:
________________________________________ Marian G. Davis 35 Palm Circle Dr. Fellings, MI 85350
Witness Signature: Name: Address:
_________________________________________ Rob Mackabee 123 Main St. Sharpsville, MI 85350
This is a RocketLawyer.com Legal Document
You might also like
- Wisconsin LLC Articles of OrganizationDocument2 pagesWisconsin LLC Articles of OrganizationRocketLawyer91% (11)
- Utah Articles of IncorporationDocument1 pageUtah Articles of IncorporationRocketLawyer83% (6)
- Tennessee LLC Articles of OrganizationDocument1 pageTennessee LLC Articles of OrganizationRocketLawyerNo ratings yet
- Delaware Certificate of IncorporationDocument3 pagesDelaware Certificate of IncorporationRocketLawyer100% (1)
- Alabama Certificate of FormationDocument4 pagesAlabama Certificate of FormationhowtoformanllcNo ratings yet
- Maine Articles of IncorporationDocument3 pagesMaine Articles of IncorporationRocketLawyer100% (1)
- Colorado LLC Articles of OrganizationDocument3 pagesColorado LLC Articles of OrganizationRocketLawyer100% (1)
- Florida Articles of IncorporationDocument4 pagesFlorida Articles of IncorporationRocketLawyer50% (2)
- Vermont Articles of OrganizationDocument1 pageVermont Articles of OrganizationRocketLawyerNo ratings yet
- Utah LLC Articles of OrganizationDocument1 pageUtah LLC Articles of OrganizationRocketLawyer100% (1)
- Colorado Articles of IncorporationDocument3 pagesColorado Articles of IncorporationRocketLawyer100% (2)
- Texas LLC Certificate of FormationDocument6 pagesTexas LLC Certificate of FormationRocketLawyer100% (5)
- Kentucky Articles of IncorporationDocument2 pagesKentucky Articles of IncorporationRocketLawyerNo ratings yet
- Arizona Articles of IncorporationDocument5 pagesArizona Articles of IncorporationRocketLawyer100% (2)
- Delaware Certificate of IncorporationDocument3 pagesDelaware Certificate of IncorporationRocketLawyer100% (1)
- South Carolina Articles of OrganizationDocument3 pagesSouth Carolina Articles of OrganizationhowtoformanllcNo ratings yet
- Ohio Articles of IncorporationDocument6 pagesOhio Articles of IncorporationRocketLawyerNo ratings yet
- West Virginia Articles of IncorporationDocument1 pageWest Virginia Articles of IncorporationRocketLawyerNo ratings yet
- New Hampshire LLC Certificate of FormationDocument5 pagesNew Hampshire LLC Certificate of FormationRocketLawyerNo ratings yet
- South Dakota Articles of OrganizationDocument3 pagesSouth Dakota Articles of OrganizationhowtoformanllcNo ratings yet
- South Carolina Articles of IncorporationDocument3 pagesSouth Carolina Articles of IncorporationRocketLawyerNo ratings yet
- Minnesota Articles of IncorporationDocument3 pagesMinnesota Articles of IncorporationRocketLawyer0% (1)
- Washington Application To Form A Profit CorporationDocument3 pagesWashington Application To Form A Profit CorporationRocketLawyer100% (2)
- Kentucky LLC Articles of OrganizationDocument2 pagesKentucky LLC Articles of OrganizationRocketLawyer100% (2)
- New Mexico LLC Articles of OrganizationDocument4 pagesNew Mexico LLC Articles of OrganizationRocketLawyer100% (1)
- Wyoming Articles of OrganizationDocument3 pagesWyoming Articles of OrganizationhowtoformanllcNo ratings yet
- Michigan LLC Articles of OrganizationDocument3 pagesMichigan LLC Articles of OrganizationRocketLawyer100% (2)
- New York Articles of IncorporationDocument2 pagesNew York Articles of IncorporationRocketLawyer100% (1)
- Arkansas Articles of IncorporationDocument2 pagesArkansas Articles of IncorporationRocketLawyer100% (1)
- Massachusetts Articles of OrganizationDocument3 pagesMassachusetts Articles of OrganizationhowtoformanllcNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ModernaDocument22 pagesModernagoslugs12No ratings yet
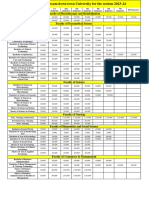
- Fees Structure Assam Down Town University For The Session 2023 2Document2 pagesFees Structure Assam Down Town University For The Session 2023 2Debashish SharmaNo ratings yet
- Jurnal Amik SanglahDocument6 pagesJurnal Amik Sanglahslamet pujianto SkepNo ratings yet
- Community Dental Health Final Flashcards - QuizletDocument19 pagesCommunity Dental Health Final Flashcards - QuizletRMNo ratings yet
- Rapid Is 2015Document11 pagesRapid Is 2015José Cunha CoutinhoNo ratings yet
- Article in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudyDocument7 pagesArticle in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudySimson TameonNo ratings yet
- Virginia HendersonDocument15 pagesVirginia Hendersondanimon1984100% (1)
- Sic PharmaDocument36 pagesSic PharmaPrakash JeswaniNo ratings yet
- Images Dickson County, TN: 2012-13Document54 pagesImages Dickson County, TN: 2012-13Journal CommunicationsNo ratings yet
- Philosophy of Nursing Service in HospitalDocument11 pagesPhilosophy of Nursing Service in HospitalAprille Sgrr100% (4)
- Modelo 1 - Parte I PDFDocument6 pagesModelo 1 - Parte I PDFandre100% (1)
- CertificateDocument1 pageCertificateLochan PhogatNo ratings yet
- Brgy. Talandang and Baganihan 2022 ConsolidatedDocument6 pagesBrgy. Talandang and Baganihan 2022 Consolidatedevelyn d. pepitoNo ratings yet
- Final Webcheck Stations Open - WebDocument6 pagesFinal Webcheck Stations Open - WebDiemut NaknanNo ratings yet
- Flow Trac SystemDocument4 pagesFlow Trac Systempolar571No ratings yet
- Bahasa Inggris - NurfadilahDocument6 pagesBahasa Inggris - NurfadilahHardianiNo ratings yet
- Health Information Exchange Fact SheetDocument4 pagesHealth Information Exchange Fact SheetDavid MarkNo ratings yet
- Types of Anesthesia ExplainedDocument3 pagesTypes of Anesthesia ExplainedJabber PaudacNo ratings yet
- Bills Approved or Enacted by Gov. McAuliffeDocument13 pagesBills Approved or Enacted by Gov. McAuliffeWSETNo ratings yet
- Inpatient DepartmentDocument7 pagesInpatient Departmentshah007zaadNo ratings yet
- Student'S Health Information Form: (E.g. Frequency, Extent, Duration, Ongoing Therapy, Etc.)Document2 pagesStudent'S Health Information Form: (E.g. Frequency, Extent, Duration, Ongoing Therapy, Etc.)Susan Loida SorianoNo ratings yet
- Module 01: Overview of Public Health Nursing in The PhilippinesDocument6 pagesModule 01: Overview of Public Health Nursing in The PhilippinesHazelNo ratings yet
- Thesis ProtocolDocument7 pagesThesis ProtocolhoneyworksNo ratings yet
- Pharma - M1L1 - Rational Drug PrescribingDocument6 pagesPharma - M1L1 - Rational Drug PrescribingEric Meynard SanchezNo ratings yet
- Public Health Nurse PHN Final Exam Past Questions For WAHEBDocument3 pagesPublic Health Nurse PHN Final Exam Past Questions For WAHEBCharles Obaleagbon86% (7)
- Comparison of Services Between Public and Private HospitalsDocument10 pagesComparison of Services Between Public and Private HospitalsJahidul IslamNo ratings yet
- Mrs. Manjushree NayakDocument3 pagesMrs. Manjushree NayakAkashNachraniNo ratings yet
- Case Study GeriaDocument12 pagesCase Study GeriaMary Grace Ogatis0% (1)
- Prevention of Avoidable Blindness and Visual ImpairmentDocument3 pagesPrevention of Avoidable Blindness and Visual ImpairmentAstidya MirantiNo ratings yet
- Receptionist: Applications Have ClosedDocument3 pagesReceptionist: Applications Have ClosedjoanmubzNo ratings yet