You might also like
- Growth and Development Failure (Failure To Thrive) Due To Parasitic InfectionsDocument49 pagesGrowth and Development Failure (Failure To Thrive) Due To Parasitic InfectionsfateeeNo ratings yet
- K1. Elektif ParasitDocument34 pagesK1. Elektif ParasitUu'ayu UnyuNo ratings yet
- Ascariasis & GiardiasisDocument34 pagesAscariasis & GiardiasisMuhammad ShahzadNo ratings yet
- Liver FluksDocument28 pagesLiver Flukszaid nabeelNo ratings yet
- Nematodes 10-11Document128 pagesNematodes 10-11microperadeniya100% (4)
- AscariasisDocument7 pagesAscariasisMia Angela Del MundoNo ratings yet
- Soil-Transmitted Helminth InfectionsDocument7 pagesSoil-Transmitted Helminth InfectionsDiane GaliNo ratings yet
- AscariasisDocument6 pagesAscariasisPika PearlasNo ratings yet
- Fascioliasis, TrematodesDocument31 pagesFascioliasis, Trematodesحسین جاسم ستارNo ratings yet
- 12 - NematodaDocument44 pages12 - NematodaAnnisya MaharaniNo ratings yet
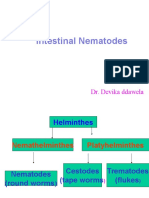
- Intestinal Nematodes: Dr. Devika DdawelaDocument127 pagesIntestinal Nematodes: Dr. Devika DdawelaPraveenKumarNo ratings yet
- Ascaris LumbricoidesDocument24 pagesAscaris LumbricoidesQonik Nuzulul FalakhiNo ratings yet
- Clinical Manifestation of AscariasisDocument28 pagesClinical Manifestation of AscariasisAishah Shalimar PutriNo ratings yet
- 2 NematodesDocument163 pages2 NematodesSammy MirandaNo ratings yet
- Food Poisoning & Worm InfestationDocument13 pagesFood Poisoning & Worm InfestationPujani SenevirathnaNo ratings yet
- HOOKWORMDocument30 pagesHOOKWORMALBINUS AmbroseNo ratings yet
- Amebiasis, Giradiasis, Helminths: DR Asim ShresthaDocument49 pagesAmebiasis, Giradiasis, Helminths: DR Asim ShresthaAsim ShresthaNo ratings yet
- Ascariasis: Roundworm Ascaris LumbricoidesDocument18 pagesAscariasis: Roundworm Ascaris LumbricoidesSuneel Kumar PrajapatiNo ratings yet
- Case Presentation: Ascariasis: Mrs. Lailanie Evangelista DotimasDocument10 pagesCase Presentation: Ascariasis: Mrs. Lailanie Evangelista DotimasRodelen MarañoNo ratings yet
- Ascari As IsDocument20 pagesAscari As IsDeladem EmmanuelNo ratings yet
- Ascari As IsDocument4 pagesAscari As IsHassan osmanNo ratings yet
- AscariasisDocument50 pagesAscariasisAnaleah MalayaoNo ratings yet
- Garima Parashar Food Poisoning PPT PR Assignment 2Document47 pagesGarima Parashar Food Poisoning PPT PR Assignment 2rahina7No ratings yet
- 01 - Parasitic Infections 2020Document85 pages01 - Parasitic Infections 2020gilbert agudoNo ratings yet
- Medical Helminthology-NematodesDocument134 pagesMedical Helminthology-NematodesKAYISIRE EMERYNo ratings yet
- Roundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandRoundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Presented by P. Jeevananth (For Award of BHMS Degree)Document66 pagesPresented by P. Jeevananth (For Award of BHMS Degree)Ajay IyerNo ratings yet
- Worm Infestation: Ms Alisha TalwarDocument82 pagesWorm Infestation: Ms Alisha TalwarSumon Kumar biswasNo ratings yet
- Parasitology: - IntroductionDocument62 pagesParasitology: - IntroductionHana AliNo ratings yet
- Kuliah 17 - Nematoda Dan ProtozoaDocument72 pagesKuliah 17 - Nematoda Dan ProtozoaivaNo ratings yet
- AscarisDocument18 pagesAscarisHabib UllahNo ratings yet
- Whip Worm (Trichuris Trichiura)Document10 pagesWhip Worm (Trichuris Trichiura)Daniel JohnsonNo ratings yet
- Intestinal Parasitic Diseases, A Simple Guide to These ConditionsFrom EverandIntestinal Parasitic Diseases, A Simple Guide to These ConditionsRating: 4 out of 5 stars4/5 (3)
- Tropical Medicine-1Document355 pagesTropical Medicine-1Fabb NelsonNo ratings yet
- Protein Energy MalnutritionDocument133 pagesProtein Energy MalnutritionMuhammad Anas AbbalNo ratings yet
- Ascaris LumbricoidesDocument33 pagesAscaris LumbricoidesRosi Gustina100% (5)
- ParasitologyLec 3 Nematodes 2 PDFDocument6 pagesParasitologyLec 3 Nematodes 2 PDFDJ RelojNo ratings yet
- Amoebiasis: (Amoebic Dysentery)Document32 pagesAmoebiasis: (Amoebic Dysentery)abhinay_1712No ratings yet
- Enterobacteriaceae:: Salmonellosis and TyphoidDocument48 pagesEnterobacteriaceae:: Salmonellosis and TyphoidPrincewill SeiyefaNo ratings yet
- AscarisDocument42 pagesAscarisمصطفي خندقاوي100% (1)
- INTESTINAL NEMATODES Hand Out 10 - 11Document6 pagesINTESTINAL NEMATODES Hand Out 10 - 11microperadeniyaNo ratings yet
- Ascaris LumbricoidesDocument33 pagesAscaris LumbricoidesBio SciencesNo ratings yet
- AphasmidsDocument60 pagesAphasmidsRitz CelsoNo ratings yet
- Cestodes: Prepared By: Charriz A. AmoyanDocument37 pagesCestodes: Prepared By: Charriz A. AmoyanAudrie Allyson GabalesNo ratings yet
- Parasitology Lec 4Document14 pagesParasitology Lec 4ao868598No ratings yet
- Ascari As IsDocument16 pagesAscari As IsCici Novelia ManurungNo ratings yet
- Nematodes: Prepared By: Charriz A. AmoyanDocument81 pagesNematodes: Prepared By: Charriz A. AmoyanAudrie Allyson GabalesNo ratings yet
- 1 DiarrheaDocument10 pages1 Diarrheaنور عزيزNo ratings yet
- Ascaris LumbricoidesDocument15 pagesAscaris LumbricoidesJyoti DasNo ratings yet
- Presented by Abhinay BhugooDocument32 pagesPresented by Abhinay BhugooGideon K. MutaiNo ratings yet
- +ascariasisDocument16 pages+ascariasisDr. SAMNo ratings yet
- Microb IntestinalDocument22 pagesMicrob IntestinalsolihinfazuniashhannasNo ratings yet
- المحاضرة 3 مادة الطفيلياتDocument5 pagesالمحاضرة 3 مادة الطفيلياتdyabw6430No ratings yet
- Lecture 7 - Parasitic Diseases - Bhunia - FS565 - 2023Document36 pagesLecture 7 - Parasitic Diseases - Bhunia - FS565 - 2023Anand KumarNo ratings yet
- COMMON WORM INFESTATION DrASBDocument54 pagesCOMMON WORM INFESTATION DrASBDr AMAL S BABUNo ratings yet
- Congenital AnomaliesDocument94 pagesCongenital AnomaliesDeepti Kukreti100% (1)
- Food Poisoning N AMOEBIASIS - LECTUREDocument60 pagesFood Poisoning N AMOEBIASIS - LECTUREpriyanka100% (1)
- Community Health Nursing: Instructor MR - Bashar Qasho'o St. Name: Bassam N. Hariri ID: 20710486Document12 pagesCommunity Health Nursing: Instructor MR - Bashar Qasho'o St. Name: Bassam N. Hariri ID: 20710486Bassam Naif HaririNo ratings yet
- Para2020 10Document46 pagesPara2020 10Koko HashamNo ratings yet
- Trichuris TrichiuraDocument3 pagesTrichuris TrichiuraTwish BeraldeNo ratings yet
- List 14 07 21Document93 pagesList 14 07 21Herowati WidjajaNo ratings yet
- Dermatofitosis 2011 1Document35 pagesDermatofitosis 2011 1Carmen Cajina Doña MamiNo ratings yet
- K-CER-001 Kylt Portfolio LD, Rev005 August2015 16 DRUCKDocument8 pagesK-CER-001 Kylt Portfolio LD, Rev005 August2015 16 DRUCKFarhan BukhariNo ratings yet
- HIV Infection in PediatricDocument36 pagesHIV Infection in PediatricFatima SaghezliNo ratings yet
- Recent Advancements in The Use of PenicillinDocument11 pagesRecent Advancements in The Use of PenicillinLokesh MahataNo ratings yet
- Quiz On ImmunizationDocument56 pagesQuiz On ImmunizationFreniNo ratings yet
- Covid 19Document1 pageCovid 19Sadiq NaseerNo ratings yet
- Peter Ho - Research PapersDocument9 pagesPeter Ho - Research Papersapi-581223483No ratings yet
- Chapter 9 - Legal and Ethical Issues in HIVAIDSDocument30 pagesChapter 9 - Legal and Ethical Issues in HIVAIDStenawNo ratings yet
- Vensim Model IndexDocument4 pagesVensim Model Indexkaren dejoNo ratings yet
- Omonigbehin Emmanuel AdedayoDocument12 pagesOmonigbehin Emmanuel AdedayoAriel GhieNo ratings yet
- Obat Antijamur: Wening Sari, DR., M.KesDocument18 pagesObat Antijamur: Wening Sari, DR., M.KesdebbyelviraNo ratings yet
- Case Ana Neonatal PneuDocument2 pagesCase Ana Neonatal PneuCharmie GandaNo ratings yet
- Hepatitis VirusesDocument19 pagesHepatitis VirusesFort SalvadorNo ratings yet
- Childhood Diarrhea Etiologies - UpToDateDocument2 pagesChildhood Diarrhea Etiologies - UpToDateLuis Emiliano ZapataNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsNiranjan WarakeNo ratings yet
- IMCI Technical Update - Including ZNDocument45 pagesIMCI Technical Update - Including ZNTinnie :)No ratings yet
- Parasite MCQDocument10 pagesParasite MCQbayati196459357950% (2)
- Aids ProjectDocument7 pagesAids Projectapi-270625016No ratings yet
- NeuroinfecciónDocument19 pagesNeuroinfecciónfabio100% (1)
- 1 WhydowefallillDocument9 pages1 WhydowefallillAbhimanyu BahreeNo ratings yet
- Are Microorganism Boon or Bane? Why?Document2 pagesAre Microorganism Boon or Bane? Why?Ellah GutierrezNo ratings yet
- Eapp Act.1Document2 pagesEapp Act.1cherish mae oconNo ratings yet
- Management of Candidemia and Invasive Candidiasis in Adults - UpToDateDocument32 pagesManagement of Candidemia and Invasive Candidiasis in Adults - UpToDatebagir_dm10No ratings yet
- DS BD MGIT TDC Identification Test BR NO en 1Document2 pagesDS BD MGIT TDC Identification Test BR NO en 1Ljuban BlanušaNo ratings yet
- 6.leptospirosis (Rev 09.16)Document22 pages6.leptospirosis (Rev 09.16)maya dwiNo ratings yet
- CarbunclesDocument15 pagesCarbunclesMr DanielNo ratings yet
- MYCOSESDocument41 pagesMYCOSESDayana PrasanthNo ratings yet
- Antibiotic TreatmentDocument25 pagesAntibiotic TreatmentNailil khusnaNo ratings yet
- Communicable Diseases QuestionsDocument11 pagesCommunicable Diseases QuestionsChelleyOllitro100% (15)