You might also like
- Pleasure CenteringDocument62 pagesPleasure Centeringemagoo100% (1)
- Operating Room Surgical ProceduresDocument197 pagesOperating Room Surgical ProceduresChin Chan100% (6)
- The Truth About Female Ejaculation Free Report1Document16 pagesThe Truth About Female Ejaculation Free Report1Thirdy HernandezNo ratings yet
- Care NewbornDocument17 pagesCare NewbornAndrea EusebiNo ratings yet
- Frogs: Body Parts and FunctionsDocument29 pagesFrogs: Body Parts and FunctionsPeeta EsdenNo ratings yet
- Children, Social Nudity and Scholarly StudyDocument3 pagesChildren, Social Nudity and Scholarly Studymjbyars200280% (5)
- Maternal Health/ OB Final Exam Study GuideDocument252 pagesMaternal Health/ OB Final Exam Study Guidelorrainenxumalo0% (2)
- MODULE 4 - 1st Part INTRAPARTAL CAREDocument15 pagesMODULE 4 - 1st Part INTRAPARTAL CARECaithlyn KirthleyNo ratings yet
- Invasive Devices On CXRDocument1 pageInvasive Devices On CXRLaurensia Erlina NataliaNo ratings yet
- Epilepsy Board Review, A Comprehensive Guide.2017 - Mohamad Z. KoubeissiDocument360 pagesEpilepsy Board Review, A Comprehensive Guide.2017 - Mohamad Z. Koubeissikaram aliNo ratings yet
- Status and Role of AYUSH and Local Health TraditionsDocument352 pagesStatus and Role of AYUSH and Local Health TraditionsSaju_Joseph_9228100% (1)
- Seminar On Preventive ObstetricsDocument50 pagesSeminar On Preventive Obstetricssalmanhabeebek85% (13)
- Home BirthDocument3 pagesHome BirthMutiara Ummu SumayyahNo ratings yet
- Incomplete Abortion MINI CASE STUDY (Group 3)Document22 pagesIncomplete Abortion MINI CASE STUDY (Group 3)Twobee Evelyn Claire62% (21)
- Maternal Test Questions 11Document10 pagesMaternal Test Questions 11dhodejun lizhalde100% (1)
- Case Pre EditedDocument112 pagesCase Pre EditedZanesville Lymont L. SubidoNo ratings yet
- Grand Case Presentation SampleDocument23 pagesGrand Case Presentation SampleWillieNo ratings yet
- Rajiv Gandhi University of Health Sciences Karnataka, BangaloreDocument22 pagesRajiv Gandhi University of Health Sciences Karnataka, BangaloreSadam HussienNo ratings yet
- Case ScenarioDocument3 pagesCase ScenarioCathy Marie Constante100% (1)
- Assignment On AmniocentesisDocument4 pagesAssignment On Amniocentesissuriya prakash100% (1)
- Preventive Obstetrics (By Mohan.s)Document52 pagesPreventive Obstetrics (By Mohan.s)mOHAN.S98% (55)
- Preventive Obstetrics PDFDocument25 pagesPreventive Obstetrics PDFAnju MargaretNo ratings yet
- DIESTRO - EINC Reaction PaperDocument2 pagesDIESTRO - EINC Reaction PaperAngela Mae DiestroNo ratings yet
- "A Strong Intention, A Relaxed Body and An Open Mind Are The Main Ingredients For An Active Birth" - Janet BalaskasDocument139 pages"A Strong Intention, A Relaxed Body and An Open Mind Are The Main Ingredients For An Active Birth" - Janet BalaskascherenjanaNo ratings yet
- Neonatal Neurology 4th Ed - G. Fenichel (Churchill Livingstone, 2007) WW PDFDocument232 pagesNeonatal Neurology 4th Ed - G. Fenichel (Churchill Livingstone, 2007) WW PDFCampan AlinaNo ratings yet
- 8 13 Draft Artikel Jurnal Dini OkDocument6 pages8 13 Draft Artikel Jurnal Dini OkIcha NaXciemonNo ratings yet
- Reike DIyah Setiawati - 042 - PSIK ADocument28 pagesReike DIyah Setiawati - 042 - PSIK ASetiaty PandiaNo ratings yet
- Gcs Prolonged Labor 1Document58 pagesGcs Prolonged Labor 1Krishane JustaleroNo ratings yet
- Individual Case Study Delivery Room Exposure: (Agusan Del Norte Provincial Hospital, Butuan City)Document13 pagesIndividual Case Study Delivery Room Exposure: (Agusan Del Norte Provincial Hospital, Butuan City)pius troy macapazNo ratings yet
- NCLEX-RN Questions: The Birth ExperienceDocument27 pagesNCLEX-RN Questions: The Birth Experienceapi-323040992No ratings yet
- MODULE 1 OB-HISTORY and OB-Physical AssesmentDocument18 pagesMODULE 1 OB-HISTORY and OB-Physical AssesmentThursten Kaye Santos SabandalNo ratings yet
- Maternal JournalDocument2 pagesMaternal JournalingridNo ratings yet
- Case Pres AutosavedDocument21 pagesCase Pres AutosavedJaysellePuguonTabijeNo ratings yet
- Analgesia For Labour: An Evidence-Based Insight For The ObstetricianDocument9 pagesAnalgesia For Labour: An Evidence-Based Insight For The ObstetricianNyeinTunNo ratings yet
- Kaloji Narayana Rao University of Health and Science, Warangal, Telangana. Proforma For The Submission of SynopsisDocument28 pagesKaloji Narayana Rao University of Health and Science, Warangal, Telangana. Proforma For The Submission of Synopsissaleha sultanaNo ratings yet
- NSDDocument44 pagesNSDabyssodeep100% (1)
- Integrated Management of Childhood IllnessDocument16 pagesIntegrated Management of Childhood IllnessSabrina Porquiado Magañan SNNo ratings yet
- Ethico-Legal Issues in The Care of Mother On Reproductive TechniquesDocument2 pagesEthico-Legal Issues in The Care of Mother On Reproductive TechniquesLiza AingelicaNo ratings yet
- Activity #1 Nupc110-CmcrpDocument4 pagesActivity #1 Nupc110-CmcrpMelody BoadoNo ratings yet
- Case Study 117Document4 pagesCase Study 117Jonah MaasinNo ratings yet
- Preoperative Evaluation and Preparation of The Gynecologic Patient - GLOWMDocument13 pagesPreoperative Evaluation and Preparation of The Gynecologic Patient - GLOWMshaliniNo ratings yet
- Childbirth Education Then and NowDocument5 pagesChildbirth Education Then and Nowazida90No ratings yet
- Case Study #117: Intrapartal CareDocument21 pagesCase Study #117: Intrapartal CareDudong SasakiNo ratings yet
- PretermDocument11 pagesPretermAlma Gobaleza100% (2)
- CADAYONA Ectopic PregnancyDocument9 pagesCADAYONA Ectopic Pregnancychn millamaNo ratings yet
- Ectopic Pregnancy Status Post Left SalpingectomyDocument37 pagesEctopic Pregnancy Status Post Left SalpingectomyAiza OronceNo ratings yet
- Seminar On PRVNTV ObgDocument43 pagesSeminar On PRVNTV Obgraghuram reddyNo ratings yet
- MODULE 3 PRENATAL CARE - Docx 1Document22 pagesMODULE 3 PRENATAL CARE - Docx 1jared abriolNo ratings yet
- Educ 100 - Activity 3Document3 pagesEduc 100 - Activity 3John Daniel DavidNo ratings yet
- Journal Reading: Advances in Understanding of Preterm BirthDocument5 pagesJournal Reading: Advances in Understanding of Preterm BirthYlamher Bufi ImperialNo ratings yet
- Assignment 1Document5 pagesAssignment 1maryamNo ratings yet
- Perineal CareDocument2 pagesPerineal CareAubrey SungaNo ratings yet
- Health Sciences Faculty Occupational School of Obstetrics: Teacher: Luis Otero QuispeDocument2 pagesHealth Sciences Faculty Occupational School of Obstetrics: Teacher: Luis Otero QuispeMarlon Castillo JaraNo ratings yet
- Anc 1 2 1Document22 pagesAnc 1 2 1Lemma AbishaNo ratings yet
- Unnecessary Prenatal Stimulation. Although There Are CommercialDocument5 pagesUnnecessary Prenatal Stimulation. Although There Are CommercialyoNo ratings yet
- Normal Spontaneous DeliveryDocument49 pagesNormal Spontaneous DeliveryA HNo ratings yet
- Preterm DeliveryDocument368 pagesPreterm DeliveryAbhishek VijayakumarNo ratings yet
- Delivery Room E-Portfolio: Bartolaba, Lyca RDocument17 pagesDelivery Room E-Portfolio: Bartolaba, Lyca RLRBNo ratings yet
- Case Study 114Document4 pagesCase Study 114Jonah MaasinNo ratings yet
- History of Present IllnessDocument30 pagesHistory of Present IllnessTrixia Joy R NachorNo ratings yet
- Care Of-Women in LabourDocument8 pagesCare Of-Women in LabourHem JoshiNo ratings yet
- Ateneo de Zamboanga University: College of Nursing Level 2Document7 pagesAteneo de Zamboanga University: College of Nursing Level 2Sheryhan Tahir BayleNo ratings yet
- Major Concerns of Women After Cesarean DeliveryDocument12 pagesMajor Concerns of Women After Cesarean DeliveryLester Gene Villegas ArevaloNo ratings yet
- Sex Sex Sex Pregnancy: Prenatal EducationDocument2 pagesSex Sex Sex Pregnancy: Prenatal EducationKevin MemoloNo ratings yet
- The Prospective Mother, a Handbook for Women During PregnancyFrom EverandThe Prospective Mother, a Handbook for Women During PregnancyNo ratings yet
- Essay 2 MartinezDocument6 pagesEssay 2 Martinezapi-644311691No ratings yet
- JournalDocument3 pagesJournalapi-740032038No ratings yet
- Nipple Pain Incidence, The Predisposing Factors, The Recovery Period After Care Management, and The Exclusive Breastfeeding OutcomeDocument5 pagesNipple Pain Incidence, The Predisposing Factors, The Recovery Period After Care Management, and The Exclusive Breastfeeding OutcomeCarmine XanderNo ratings yet
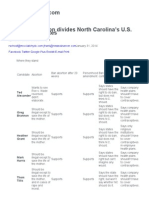
- North Carolina's GOP Candidates For US Senate Strongly Oppose Women's RightsDocument5 pagesNorth Carolina's GOP Candidates For US Senate Strongly Oppose Women's Rightsmjbyars2002No ratings yet
- WinstonDocument2 pagesWinstonNew York PostNo ratings yet
- Nightmare in Maryville Teens' Sexual Encounter Ignites A Firestorm Against FamilyDocument8 pagesNightmare in Maryville Teens' Sexual Encounter Ignites A Firestorm Against Familymjbyars2002No ratings yet
- B-Inggris YesDocument3 pagesB-Inggris YesdadansuryawanNo ratings yet
- Kayedeke Barbara Updated CVDocument4 pagesKayedeke Barbara Updated CVRichard OkelloNo ratings yet
- Guidelines For Amniocentesis and Chorionic Villus Sampling 2009Document8 pagesGuidelines For Amniocentesis and Chorionic Villus Sampling 2009Atik ShaikhNo ratings yet
- STS, MoneraDocument7 pagesSTS, MoneraJohn Philip MoneraNo ratings yet
- Evolution in Tissue Expander Design For Breast Reconstruction: Technological Innovation To Optimize Patient OutcomesDocument10 pagesEvolution in Tissue Expander Design For Breast Reconstruction: Technological Innovation To Optimize Patient OutcomesFauzi Novia Isnaening TyasNo ratings yet
- HB 12-1300 - Professional Review Committees FactSheetDocument2 pagesHB 12-1300 - Professional Review Committees FactSheetSenator Mike JohnstonNo ratings yet
- Teladoc Member: Frequently Asked QuestionsDocument2 pagesTeladoc Member: Frequently Asked QuestionsGenesis LopezNo ratings yet
- Hygiene Sanitasi Organ Genetalia WanitaDocument25 pagesHygiene Sanitasi Organ Genetalia WanitaYunita Tri JayatiNo ratings yet
- WWW Scribd Com Document 437023289 Polyhydramnios CASE STUDYDocument14 pagesWWW Scribd Com Document 437023289 Polyhydramnios CASE STUDYJv LalparaNo ratings yet
- Accu Chek Reference Guide Blood Glucose Monitor 98 79 EC 3969Document63 pagesAccu Chek Reference Guide Blood Glucose Monitor 98 79 EC 3969k1971No ratings yet
- GRE Word RootsDocument28 pagesGRE Word Rootshacker17No ratings yet
- Background Results: DR Aditya Bhat, DR, Amit Misri Department of Paediatric Cardiology, Medanta-The Medicity, GurgaonDocument1 pageBackground Results: DR Aditya Bhat, DR, Amit Misri Department of Paediatric Cardiology, Medanta-The Medicity, GurgaonADNo ratings yet
- Elastomeric Impression TechniquesDocument60 pagesElastomeric Impression TechniquesAnupriya SinghNo ratings yet
- Fertility and Sterility Treating Hydrosalpinx With A Manual Physical TherapyDocument1 pageFertility and Sterility Treating Hydrosalpinx With A Manual Physical TherapyClearPassageNo ratings yet
- Vulvar ProceduresDocument14 pagesVulvar Proceduresjft842No ratings yet
- Critical Appraisal PROGNOSIS Jurnal ReadingDocument5 pagesCritical Appraisal PROGNOSIS Jurnal Readingsiekasmat upaNo ratings yet
- Obstetric by 10 Teachers Chapter 8Document25 pagesObstetric by 10 Teachers Chapter 8FerasNo ratings yet
- Hospital Emergency Department Facility Audit Report - OT, Ward and Floor ManagementDocument12 pagesHospital Emergency Department Facility Audit Report - OT, Ward and Floor Managementjeremy joshuaNo ratings yet
- NCM 107 Skills LaboratoryDocument27 pagesNCM 107 Skills LaboratoryCharlmagne LinnamNo ratings yet
- Prom PromDocument33 pagesProm PromMichelle HendrayantaNo ratings yet