You might also like
- Mary Bond - The Pelvic LiftDocument4 pagesMary Bond - The Pelvic Liftleo100% (1)
- Rolfing & YogaDocument2 pagesRolfing & Yogal_auracNo ratings yet
- Rolf HingesDocument8 pagesRolf Hingeswalterego58100% (3)
- Master your myofascial meridiansDocument6 pagesMaster your myofascial meridiansEldar SulejmanovicNo ratings yet
- Training ProgramDocument31 pagesTraining ProgramBroadway BluesNo ratings yet
- IFF AY Lesson IndexDocument30 pagesIFF AY Lesson IndexPaulina Chirif Camino100% (1)
- Diaphragmatic BreathDocument10 pagesDiaphragmatic BreathPhooi Yee LauNo ratings yet
- Dental equilibration, osteopathy, and temporomandibular joint dysfunctionDocument9 pagesDental equilibration, osteopathy, and temporomandibular joint dysfunctionshivnairNo ratings yet
- Visceral Patterns in ScoliDocument4 pagesVisceral Patterns in ScolileoNo ratings yet
- Fingers Feldenkrais 333Document9 pagesFingers Feldenkrais 333Anonymous edr05e7INo ratings yet
- Alexander Technique and Feldenkrais MethodDocument2 pagesAlexander Technique and Feldenkrais MethodAlfonso Aguirre DergalNo ratings yet
- The World's Greatest Stretch SeriesDocument1 pageThe World's Greatest Stretch SeriesRoberto HernandezNo ratings yet
- Body Awareness and MovementDocument6 pagesBody Awareness and Movementapi-297150429No ratings yet
- 2014 SAAO Forum For 10-18-11 Cranial IntroDocument5 pages2014 SAAO Forum For 10-18-11 Cranial IntroRoger NakataNo ratings yet
- 2013 Perth 3 Course - GuideDocument38 pages2013 Perth 3 Course - GuideDori BarreirosNo ratings yet
- Sleeping Positions and Their Impact on HealthDocument68 pagesSleeping Positions and Their Impact on Healthgabitor100% (1)
- Posture in ActionDocument0 pagesPosture in ActionMrJabberwockijacks100% (3)
- Rolfing Concepts PDFDocument14 pagesRolfing Concepts PDFdavidescu5costinNo ratings yet
- Pilates and The Powerhouse II PDFDocument9 pagesPilates and The Powerhouse II PDFviboramorNo ratings yet
- HEWES, Gordon. World Distribution of Certain Postural HabitsDocument14 pagesHEWES, Gordon. World Distribution of Certain Postural Habitsrogerio_felix_38No ratings yet
- FeldenkraisDocument120 pagesFeldenkraiskukutxiNo ratings yet
- Alexander Breathing Pain ReliefDocument2 pagesAlexander Breathing Pain ReliefSyedNo ratings yet
- What is Psycho-Peristalsis and How it Relates to HealingDocument5 pagesWhat is Psycho-Peristalsis and How it Relates to HealingneredehangiNo ratings yet
- SomaticsColorCatalog5 4 06Document17 pagesSomaticsColorCatalog5 4 06Viviana PueblaNo ratings yet
- The Feldenkrais Method IntroductionDocument3 pagesThe Feldenkrais Method IntroductionWangshosan100% (3)
- Kevin Frank - Body - As - A - Movement - SystemDocument10 pagesKevin Frank - Body - As - A - Movement - SystemleoNo ratings yet
- Eldoa Lesson PlanDocument3 pagesEldoa Lesson Planapi-359540985No ratings yet
- Yoga For KyphosisDocument13 pagesYoga For KyphosisLaerte100% (1)
- Chapter 1Document12 pagesChapter 1mohitnet1327No ratings yet
- Nerve Glides English VersionDocument4 pagesNerve Glides English VersionraseelNo ratings yet
- Ligamentous Articular Strain - Osteopathic ManipulativeDocument20 pagesLigamentous Articular Strain - Osteopathic Manipulativeisa_martínezNo ratings yet
- Alexander Technique and Feldenkrais Method: A CriticalDocument16 pagesAlexander Technique and Feldenkrais Method: A CriticalAna Carolina PetrusNo ratings yet
- Diagnostic Touch Parts I IV by Rollin Becker PDFDocument69 pagesDiagnostic Touch Parts I IV by Rollin Becker PDFCatalin EneNo ratings yet
- Dr. Moshe Feldenkrais - Alexander Yanai Lessons (Volume 5)Document373 pagesDr. Moshe Feldenkrais - Alexander Yanai Lessons (Volume 5)Cherry100% (1)
- KinesiologyDocument4 pagesKinesiologyJulie Brookelle Jacquinot100% (1)
- Neutral spine principle may aid rehabilitationDocument12 pagesNeutral spine principle may aid rehabilitationsabrina100% (1)
- Ankle Muscles PDFDocument85 pagesAnkle Muscles PDFFanny Indra WarmanNo ratings yet
- Ligaments Positional ReleaseDocument2 pagesLigaments Positional ReleaseFlorence LeoNo ratings yet
- Sacrum TechniquesDocument3 pagesSacrum Techniquesiruizmolina100% (1)
- Wedel PDFDocument120 pagesWedel PDFAbhishek VermaNo ratings yet
- Basic Anatomy TrainsDocument8 pagesBasic Anatomy TrainsJ FNo ratings yet
- TIFF 2023 Programme Book - Online Edition - 17 Aug 2023Document324 pagesTIFF 2023 Programme Book - Online Edition - 17 Aug 2023CathyNo ratings yet
- Psychosynthesis Quarterly March 2017Document60 pagesPsychosynthesis Quarterly March 2017SFLegionNo ratings yet
- Feldenkrais Exercise For Neck and Shoulder PainDocument20 pagesFeldenkrais Exercise For Neck and Shoulder PainCarmen Llerenas100% (3)
- Banton BiomechanicsDocument9 pagesBanton BiomechanicsIoan AndraNo ratings yet
- Master The Pike - ForumsDocument4 pagesMaster The Pike - ForumsJacklynlim LkcNo ratings yet
- Entrainement and The Cranial Rythmic ImpulseDocument7 pagesEntrainement and The Cranial Rythmic ImpulseDenise Mathre100% (1)
- Advanced Muscle Integration TechniqueDocument4 pagesAdvanced Muscle Integration Techniquepatsim0% (1)
- Bodily Expressions Moshe FeldenkraisDocument10 pagesBodily Expressions Moshe FeldenkraisPatricia Isabel FrancoNo ratings yet
- Feldenkrais Unstable EquilibriumDocument15 pagesFeldenkrais Unstable Equilibriumvk100% (1)
- Self Myofascial ReleaseDocument22 pagesSelf Myofascial ReleaseMuhammad Fahmy100% (1)
- Free Yourself From Back PainDocument44 pagesFree Yourself From Back PainSteveLangNo ratings yet
- What Is TinnitusDocument6 pagesWhat Is TinnitusAdrian TangNo ratings yet
- Hold the foot firmly in dorsiflexion to relax the gastrocnemiusmuscle and expose the Achilles tendon fullyDocument13 pagesHold the foot firmly in dorsiflexion to relax the gastrocnemiusmuscle and expose the Achilles tendon fullyNurul Huda M ShahrinNo ratings yet
- The Feldenkrais Method - Application, Practice and PrinciplesDocument8 pagesThe Feldenkrais Method - Application, Practice and PrinciplesPaul Asturbiaris100% (1)
- Spirit in Motion: Gym & Water Fitness / Yoga Breath-Stretch TechniqueFrom EverandSpirit in Motion: Gym & Water Fitness / Yoga Breath-Stretch TechniqueNo ratings yet
- Movement work according to Elsa Gindler: working with the feetFrom EverandMovement work according to Elsa Gindler: working with the feetNo ratings yet
- Chin Up KinesiologyDocument6 pagesChin Up KinesiologyMoffOmbasa100% (2)
- Amyporterfield TWN ExitrunwaychecklistDocument3 pagesAmyporterfield TWN Exitrunwaychecklistbackch9011No ratings yet
- Studio Microphones - in Store and Online - Turramurra MusicDocument32 pagesStudio Microphones - in Store and Online - Turramurra Musicbackch9011No ratings yet
- Luxaflex - Products - External Collection - Folding Arm Awnings - BrochureDocument20 pagesLuxaflex - Products - External Collection - Folding Arm Awnings - Brochurebackch9011No ratings yet
- Minor Fall Major LiftDocument11 pagesMinor Fall Major Liftbackch9011No ratings yet
- Writers festival-PROGRAM-0219 PDFDocument20 pagesWriters festival-PROGRAM-0219 PDFbackch9011No ratings yet
- Full ScaleDocument1 pageFull Scalebackch9011No ratings yet
- Tortex - Guitar Picks - ProductsDocument8 pagesTortex - Guitar Picks - Productsbackch9011No ratings yet
- NIMA Membership Form 2019Document2 pagesNIMA Membership Form 2019backch9011No ratings yet
- Toontrack Superior Drummer 3Document11 pagesToontrack Superior Drummer 3backch9011100% (1)
- Folding Arm Awnings - Care & CleaningDocument4 pagesFolding Arm Awnings - Care & Cleaningbackch9011No ratings yet
- The Sound of The Next Generation - Final Spread PDFDocument17 pagesThe Sound of The Next Generation - Final Spread PDFbackch9011No ratings yet
- THOR0028 Catalogue WWW 1Document52 pagesTHOR0028 Catalogue WWW 1backch90110% (1)
- General MidiDocument9 pagesGeneral Midibackch9011No ratings yet
- Grammy Award For Producer of The Year, Non-Classical - WikipediaDocument1 pageGrammy Award For Producer of The Year, Non-Classical - Wikipediabackch9011No ratings yet
- Social Media For MusiciansDocument24 pagesSocial Media For MusiciansTuneCore100% (1)
- Grammy Award For Producer of The Year, Non-Classical - WikipediaDocument1 pageGrammy Award For Producer of The Year, Non-Classical - Wikipediabackch9011No ratings yet
- ARIA Award For Engineer of The Year - WikipediaDocument6 pagesARIA Award For Engineer of The Year - Wikipediabackch9011No ratings yet
- Getting Started Getting StartedDocument1 pageGetting Started Getting Startedbackch9011No ratings yet
- Fantom HelpDocument2 pagesFantom Helpbackch9011No ratings yet
- Resident Visitor Parking Application FormDocument2 pagesResident Visitor Parking Application Formbackch9011No ratings yet
- ASIO4ALL v2 Instruction ManualDocument11 pagesASIO4ALL v2 Instruction ManualDanny_Grafix_1728No ratings yet
- ARIA Award For Producer of The Year - WikipediaDocument6 pagesARIA Award For Producer of The Year - Wikipediabackch9011No ratings yet
- May 2018 - Program Fact Sheet For Neis FinalDocument2 pagesMay 2018 - Program Fact Sheet For Neis Finalbackch9011No ratings yet
- VR AnagramsDocument22 pagesVR Anagramsbackch9011No ratings yet
- Ecco Beverage Aug18Document7 pagesEcco Beverage Aug18backch9011No ratings yet
- Ecco Alcarte 011118Document1 pageEcco Alcarte 011118backch9011No ratings yet
- Yamaha Acoustic Guitar Archive v6.4.3 Excel 97 2003Document238 pagesYamaha Acoustic Guitar Archive v6.4.3 Excel 97 2003backch90110% (1)
- Chefs Menu December 2018: Aperitif Suggestions BlushDocument1 pageChefs Menu December 2018: Aperitif Suggestions Blushbackch9011No ratings yet
- BAUHN AMCD-415+-+Instruction+Manual Tablet Smartphone Mirroring DongleDocument28 pagesBAUHN AMCD-415+-+Instruction+Manual Tablet Smartphone Mirroring Donglebackch9011No ratings yet
- Ecco Wine 081218Document2 pagesEcco Wine 081218backch9011No ratings yet
- KO2014 outlinesENGDocument11 pagesKO2014 outlinesENGjudo1klub1slovenj1grNo ratings yet
- Mazaka BrochureDocument4 pagesMazaka BrochureJavicontryNo ratings yet
- Laws of The Game 2018 19 PDFDocument228 pagesLaws of The Game 2018 19 PDFAlex ManoleNo ratings yet
- Volvo S60 2002Document63 pagesVolvo S60 2002Mac PirxNo ratings yet
- Kirloskar Pump 4R1040 Maintenance SheetDocument95 pagesKirloskar Pump 4R1040 Maintenance SheetArun ShyamrajNo ratings yet
- Sizes: Zodiac Hurricane: Critical Mission SolutionsDocument2 pagesSizes: Zodiac Hurricane: Critical Mission SolutionsEtrcilNo ratings yet
- GRPEX14-Assignment (Release 2) - 2-2Document15 pagesGRPEX14-Assignment (Release 2) - 2-2EllaNo ratings yet
- Bach - Fugue From Violin Sonata N. 1 (BWV 1001)Document8 pagesBach - Fugue From Violin Sonata N. 1 (BWV 1001)Satoshi IdeNo ratings yet
- Rifle Recoil ChartDocument6 pagesRifle Recoil Chartblowmeasshole1911No ratings yet
- Gns03 Realms of Terrinoth Lesser EvilsDocument41 pagesGns03 Realms of Terrinoth Lesser EvilsJeremieHunter100% (2)
- DemosceneDocument17 pagesDemosceneYiddam QuiriarteNo ratings yet
- AmiiboDocument211 pagesAmiibomikepelenskyNo ratings yet
- GRUNDFOS INSTRUCTIONS MULTIlift M/MD AND MOGDocument7 pagesGRUNDFOS INSTRUCTIONS MULTIlift M/MD AND MOGParveez HusnooNo ratings yet
- Dr. Tommy SP - BS - Head Trauma Webinar Dr. TMYDocument30 pagesDr. Tommy SP - BS - Head Trauma Webinar Dr. TMYOctafiani Trikartika DarimanNo ratings yet
- Complete 10 Day Volleyball UnitDocument25 pagesComplete 10 Day Volleyball UnitJane Nherica UddipaNo ratings yet
- Premium Fuel Case Study Squash TournamentDocument2 pagesPremium Fuel Case Study Squash TournamentAmbarish AdhikariNo ratings yet
- Becker Orthometry FormsDocument13 pagesBecker Orthometry FormslauelvNo ratings yet
- 0900 - 1078 - 00 C500 D5 (QSX15G8 With PCC2100) : Issue 01 20/02/06 Initial IssueDocument2 pages0900 - 1078 - 00 C500 D5 (QSX15G8 With PCC2100) : Issue 01 20/02/06 Initial IssueEdgar RamirezNo ratings yet
- Zamar Valley MapDocument1 pageZamar Valley MapMuhammad Usman100% (2)
- SORRCA Rules & Specs for Scale Off-Road RC CompetitionsDocument6 pagesSORRCA Rules & Specs for Scale Off-Road RC CompetitionsDeeds VillapandoNo ratings yet
- Rogue Trader - Soul Reaver Character SheetDocument2 pagesRogue Trader - Soul Reaver Character SheetGeorges GodfroyNo ratings yet
- Guide To The Books of BaroviaDocument3 pagesGuide To The Books of BaroviavolthurNo ratings yet
- Zf6 6r60 Zip BookletDocument8 pagesZf6 6r60 Zip BookletPablo Farfan Alvarez100% (1)
- Hello World The Match Is in ProgressDocument31 pagesHello World The Match Is in ProgressRubel RanaNo ratings yet
- 101 Purchase Request: Responsibility Center CodeDocument1 page101 Purchase Request: Responsibility Center CodeRosalie Cotillar BaldezamoNo ratings yet
- Mowing: Job Safety Analysis Mowing Operation Mowing With A Zero Turn or Riding LawnmowerDocument2 pagesMowing: Job Safety Analysis Mowing Operation Mowing With A Zero Turn or Riding LawnmowerRetselisitsoe100% (1)
- (Free Scores - Com) - Kondo Koji Mario Bros Theme Song Bass Clarinet 32398 PDFDocument2 pages(Free Scores - Com) - Kondo Koji Mario Bros Theme Song Bass Clarinet 32398 PDFEdgar VillanuevaNo ratings yet
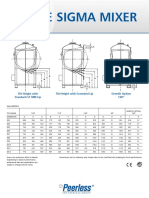
- Sigma MixerDocument2 pagesSigma Mixermmk111No ratings yet
- STRONG Fitness Magazine 2013-11-12Document82 pagesSTRONG Fitness Magazine 2013-11-12Arturo FloresNo ratings yet
- Gymnastics Lesson PlanDocument10 pagesGymnastics Lesson Planapi-486232490No ratings yet