You might also like
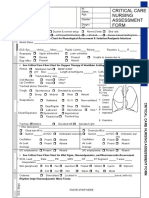
- Critical Care Nursing Assessment Form: R R R R R R R RDocument2 pagesCritical Care Nursing Assessment Form: R R R R R R R RPipit Permata100% (1)
- Blank Basic Nursing Physical AssessmentDocument1 pageBlank Basic Nursing Physical AssessmentAmeliaM100% (3)
- Critical Care Notes BookDocument142 pagesCritical Care Notes BookDerick RanaNo ratings yet
- Critical Care NursingDocument159 pagesCritical Care NursingJoy Jarin50% (2)
- Morse Fall Risk Assessment ToolDocument2 pagesMorse Fall Risk Assessment ToolDinar Chieko100% (1)
- RN Critical Care Competency ChecklistDocument19 pagesRN Critical Care Competency ChecklistMary ElizabethNo ratings yet
- Idoc - Pub - Critical Care Nursing Assessment FormDocument3 pagesIdoc - Pub - Critical Care Nursing Assessment FormNamra AnsariNo ratings yet
- Critical Care Nurse Skills ChecklistDocument4 pagesCritical Care Nurse Skills ChecklistMichael Silva0% (1)
- Critical Care Nursing Course MapDocument1 pageCritical Care Nursing Course MapMelissa David0% (1)
- Acute Critical Care Nursing HandoutDocument17 pagesAcute Critical Care Nursing HandoutJulie May100% (6)
- Emergency Nurse OrientationDocument3 pagesEmergency Nurse Orientationani mulyaniNo ratings yet
- Critical Care NursingDocument10 pagesCritical Care Nursingianecunar100% (10)
- Nurse Assessment ChecklistDocument3 pagesNurse Assessment Checklistclarimer100% (3)
- CEN+Online+Review Module+12 Final GENITODocument26 pagesCEN+Online+Review Module+12 Final GENITOTamara Cooper67% (3)
- Skills Checklist-Critical CareDocument3 pagesSkills Checklist-Critical CareRom Anog100% (4)
- Drug Study ICUDocument14 pagesDrug Study ICUAndrea Isabel U. O'DellNo ratings yet
- Nurse Brain Sheet With Shift HoursDocument2 pagesNurse Brain Sheet With Shift HoursLauren Cournoyer Foreman100% (4)
- ICU Nurse Report SheetDocument1 pageICU Nurse Report SheetPuteri Hutami50% (4)
- Adult Critical Care Nursing Knowledge & Skills ChecklistDocument7 pagesAdult Critical Care Nursing Knowledge & Skills Checklistnorthweststaffing100% (3)
- Nursing "Brains" Report Sheet 4Document1 pageNursing "Brains" Report Sheet 4girlywhirl100% (2)
- Float Pool - Orientation - RN Critical Care Competency ChecklistDocument19 pagesFloat Pool - Orientation - RN Critical Care Competency Checklistpurwadis100% (2)
- Emergency Room Nursing Knowledge & Skills ChecklistDocument3 pagesEmergency Room Nursing Knowledge & Skills Checklistnorthweststaffing100% (1)
- Critical Care Nursing Notes 2 - Med SurgDocument42 pagesCritical Care Nursing Notes 2 - Med Surgpauchanmnl100% (3)
- Chart Smart - The a-To-Z Guide 3rdDocument507 pagesChart Smart - The a-To-Z Guide 3rdDanae Jones100% (2)
- OTM 1.04 Nursing Brainsheet DatabaseDocument46 pagesOTM 1.04 Nursing Brainsheet Databaserachel loren100% (7)
- ICU/CCU Only Competencies and Johns Hopkins MHA ICU ProjectDocument107 pagesICU/CCU Only Competencies and Johns Hopkins MHA ICU Projecthery100% (2)
- SBAR - Template PDFDocument5 pagesSBAR - Template PDFHosam GomaaNo ratings yet
- Competency For O.R. NursesDocument9 pagesCompetency For O.R. NursesRomeo Santarina67% (3)
- Study Guide Emergency and Trauma NursingDocument11 pagesStudy Guide Emergency and Trauma NursingMarie Angelique Cruz Crestani100% (5)
- Physical Assessment Charting For NursingDocument7 pagesPhysical Assessment Charting For NursingChristine Schroeder92% (13)
- CriticalCare - ICU Skills ChecklistDocument8 pagesCriticalCare - ICU Skills Checklistyash Inficare100% (2)
- Icu Nurse Crash CourseDocument3 pagesIcu Nurse Crash CourseSERA B.100% (2)
- Vsim Case Sara Lin Virtual ClinicalDocument12 pagesVsim Case Sara Lin Virtual ClinicalLivan Martell100% (4)
- 8 Week CCRN Study PlanDocument6 pages8 Week CCRN Study PlanJoshua Atienza100% (2)
- CCRN Exam CramDocument2 pagesCCRN Exam CramJan Marcus0% (3)
- 17 Tips To Improve Your Nursing DocumentationDocument26 pages17 Tips To Improve Your Nursing DocumentationAgustin Lutfiana100% (1)
- Head To Toe Assessment Guide PDFDocument6 pagesHead To Toe Assessment Guide PDFTashaNo ratings yet
- Critical Care Nursing Manuall IDocument90 pagesCritical Care Nursing Manuall ILesley Gonzalez75% (4)
- Comprehensive physical exam findingsDocument3 pagesComprehensive physical exam findingsCatherine Drew Sims100% (6)
- MRN: - Weight: - KG Age: - : Risk/RestraintDocument2 pagesMRN: - Weight: - KG Age: - : Risk/Restraintrustiejade100% (3)
- Psychiatric Nursing Knowledge and Skills ChecklistDocument5 pagesPsychiatric Nursing Knowledge and Skills Checklistnorthweststaffing100% (4)
- Organizing Patient CareDocument18 pagesOrganizing Patient CareAqmarindaLailyaGhassani80% (5)
- Nursing Report Sheet (Revised For Neuro)Document1 pageNursing Report Sheet (Revised For Neuro)HayleyLangley100% (4)
- Critical Care Nursing A Holistic Approach 10th Edition Morton Test Bank PDFDocument6 pagesCritical Care Nursing A Holistic Approach 10th Edition Morton Test Bank PDFa806088253No ratings yet
- Role of Critical Care Nurses in Caring for Critically Ill PatientsDocument10 pagesRole of Critical Care Nurses in Caring for Critically Ill PatientsHanis Rozib99% (69)
- Icu GuidebookDocument43 pagesIcu Guidebookdrimran570100% (4)
- Assessment of The Critically Ill Patients and Their FamiliesDocument48 pagesAssessment of The Critically Ill Patients and Their Familiesjhing_apdan100% (1)
- AHA GWTG-R Code Blue Documentation FormDocument3 pagesAHA GWTG-R Code Blue Documentation Formrubertusedy100% (3)
- TNCC Prep Packet Revised June 2016Document12 pagesTNCC Prep Packet Revised June 2016nurse2012100% (3)
- Code Blue Running SheetDocument2 pagesCode Blue Running Sheetenumula kumar100% (11)
- Nurse Report Sheet SBARDocument4 pagesNurse Report Sheet SBARBryan Nguyen50% (2)
- Ccrn Certification Examination Practice Questions and Answers with Rationale: First EditionFrom EverandCcrn Certification Examination Practice Questions and Answers with Rationale: First EditionRating: 5 out of 5 stars5/5 (1)
- Adult CCRN Exam Premium: For the Latest Exam Blueprint, Includes 3 Practice Tests, Comprehensive Review, and Online Study PrepFrom EverandAdult CCRN Exam Premium: For the Latest Exam Blueprint, Includes 3 Practice Tests, Comprehensive Review, and Online Study PrepNo ratings yet
- Surviving the ICU: A Toolkit for the Critical Care NurseFrom EverandSurviving the ICU: A Toolkit for the Critical Care NurseNo ratings yet
- Adult CCRN Exam Flashcards, Second Edition: Up-to-Date Review and PracticeFrom EverandAdult CCRN Exam Flashcards, Second Edition: Up-to-Date Review and PracticeRating: 5 out of 5 stars5/5 (1)
- Easy Nursing Notes For The Registered Nurse.From EverandEasy Nursing Notes For The Registered Nurse.Rating: 4 out of 5 stars4/5 (6)
- 3M Half Facepiece Respirator 6000 Series User InstructionsDocument2 pages3M Half Facepiece Respirator 6000 Series User InstructionsPaola Millare - MuharraniNo ratings yet
- Hempadur 85675 Base 8567510000 En-UsDocument9 pagesHempadur 85675 Base 8567510000 En-UsAllan LindoNo ratings yet
- Bawalan, Hewlett Pearl L. February 11, 2021 Module 4: AsthmaDocument5 pagesBawalan, Hewlett Pearl L. February 11, 2021 Module 4: AsthmaHewlett Pearl BawalanNo ratings yet
- G 3 NCM 122 Lab BSN 4 2 FinalDocument67 pagesG 3 NCM 122 Lab BSN 4 2 FinalPam RomeroNo ratings yet
- Vital Signs NotesDocument3 pagesVital Signs NotesJoelyn Noble CabalatunganNo ratings yet
- Focus/ Nursing Diagnosis Data Action Response: Discharge PlanningDocument2 pagesFocus/ Nursing Diagnosis Data Action Response: Discharge PlanningJasonlee BaluyotNo ratings yet
- CHEST 6. Chest Trauma 2022 YismawDocument61 pagesCHEST 6. Chest Trauma 2022 YismawrobelNo ratings yet
- Human Body WebQuestDocument6 pagesHuman Body WebQuestjennyferchoNo ratings yet
- Naso Gastric Tubes QuestionsDocument5 pagesNaso Gastric Tubes QuestionsjhonNo ratings yet
- Caffeine MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesCaffeine MSDS: Section 1: Chemical Product and Company IdentificationAnglila Diebi SalmaputriNo ratings yet
- L-Glutamic Acid MSDS: Section 1: Chemical Product and Company IdentificationDocument5 pagesL-Glutamic Acid MSDS: Section 1: Chemical Product and Company IdentificationpipitfpuspitaNo ratings yet
- 05-06-2021 HMB EnglishDocument66 pages05-06-2021 HMB EnglishKiran SNNo ratings yet
- Twisting Flow Yoga Sequence A4 FREEDocument1 pageTwisting Flow Yoga Sequence A4 FREEmateriaelementalNo ratings yet
- Atls FlashcardDocument74 pagesAtls FlashcardAzis Aai92% (71)
- SAFETY DATA SHEET for MAGNETIC PARTICLE SUSPENSIONDocument6 pagesSAFETY DATA SHEET for MAGNETIC PARTICLE SUSPENSIONazam RazzaqNo ratings yet
- Apply Medical First Aid On Board Ship PDFDocument152 pagesApply Medical First Aid On Board Ship PDFNovi Indah LestariNo ratings yet
- Ventilation Horse Barns and Stable DesignDocument50 pagesVentilation Horse Barns and Stable DesignQOBIT100% (2)
- Marie Antoniette F. AbsalonDocument48 pagesMarie Antoniette F. AbsalonMarie Antoniette AbsalonNo ratings yet
- Babylog-Vn500 With HFODocument10 pagesBabylog-Vn500 With HFOABHINANDAN SHARMANo ratings yet
- CPR Guidelines During COVID-19Document2 pagesCPR Guidelines During COVID-19Arabind Ach AryaNo ratings yet
- 03-12-2020 HMB EnglishDocument10 pages03-12-2020 HMB EnglishKiran SNNo ratings yet
- Data Ruangan Intensive (071020)Document31 pagesData Ruangan Intensive (071020)Andrew WarankiranNo ratings yet
- Vaccine Report LatestDocument2 pagesVaccine Report LatestEmmanuel DemostheneNo ratings yet
- Endotracheal Intubation and Treacheastomy.Document9 pagesEndotracheal Intubation and Treacheastomy.Savita HanamsagarNo ratings yet
- Cosmic Sounds - Sounds That Heal PDFDocument50 pagesCosmic Sounds - Sounds That Heal PDFAlexandra Ioana Niculescu50% (2)
- Aeon7200 Anesthesia Machine: Configuration Price List (v1.00)Document7 pagesAeon7200 Anesthesia Machine: Configuration Price List (v1.00)PABLO ZAMUDIONo ratings yet
- The Affirmations of L. Ron HubbardDocument29 pagesThe Affirmations of L. Ron HubbardThe Department of Official InformationNo ratings yet
- MDI Use in 4 StepsDocument4 pagesMDI Use in 4 Stepsarn0ld21No ratings yet
- Acute Respiratory Distress Syndrome: By: Ben Meron MichalDocument13 pagesAcute Respiratory Distress Syndrome: By: Ben Meron Michalmichal ben meronNo ratings yet
- CURB-65 Pneumonia Severity Score: CURB-65 Score 0-1 Points: Low Risk 2-5 Points: Higher RiskDocument1 pageCURB-65 Pneumonia Severity Score: CURB-65 Score 0-1 Points: Low Risk 2-5 Points: Higher RiskErinNo ratings yet